Kato Shingo, Teixeira Bruno Casaes, Laurent Thomas, Yamada Yoshiyuki, Dave Kiran, Shah Shweta, Kim Hyunchung
Saitama Medical Center, Saitama Medical University, Saitama, Japan.
Bristol Myers Squibb, London, UK.
Adv Ther. 2025 Mar;42(3):1435-1447. doi: 10.1007/s12325-024-03096-1. Epub 2025 Jan 24.
This retrospective claims analysis characterized contemporary ulcerative colitis (UC) treatment patterns and investigated the economic burden of UC in Japan.
This study used anonymized claims data in the Medical Data Vision database. Patients were included if they had a confirmed UC diagnosis and ≥ 1 claim of systemic treatment for UC (index date) between June 2018 and December 2022, in addition to continuous enrollment for ≥ 6 months before and ≥ 12 months after the index date. Patients were excluded if they were aged < 18 years at index or if they had claimed systemic UC treatment during the pre-index period, had a confirmed diagnosis of Crohn's or Behçet's disease, or had a record of colectomy during the pre-index period. Outcomes of interest were treatment patterns, healthcare resource utilization (HCRU), and UC-related costs per person per month (PPPM). Further exploratory analyses were conducted to understand whether real-world treatment patterns with conventional therapy were optimally aligned with guideline recommendations. Two definitions of suboptimal treatment with conventional therapies were identified: prolonged treatment with corticosteroids (i.e., consecutive use for > 90 days) and corticosteroid cycling (i.e., three or more ≥ 30-day corticosteroid courses over 1 year, with a ≥ 60-day gap between courses).
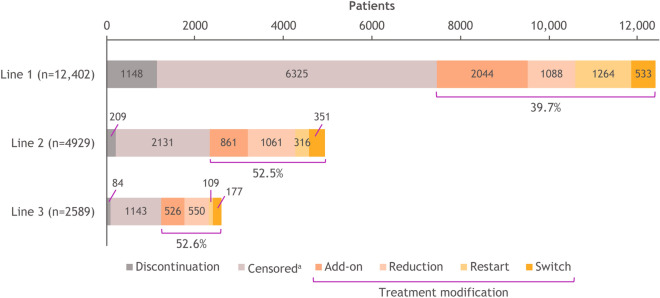
Overall, 15,429 patients were included. The most frequently observed class of first-line treatment was 5-aminosalicylic acid monotherapy (75.0%); treatment modification was observed in 39.7% of patients. Within 1 year of follow-up, patients had a mean (SD) of 9.8 (6.8) outpatient visits, and a hospital stay was reported in 23.9% of patients. Mean total cost PPPM was ¥76,374. Of patients with ≥ 1 course of corticosteroids, 39.8% received suboptimal treatment with conventional therapies. HCRU and total costs were higher for patients with versus without suboptimal treatment with conventional therapies.
Japanese patients with UC would benefit from treatment options that can reduce costs, HCRU, and suboptimal treatment with conventional therapies.
本回顾性索赔分析描述了当代溃疡性结肠炎(UC)的治疗模式,并调查了日本UC的经济负担。
本研究使用了医疗数据愿景数据库中的匿名索赔数据。纳入标准为在2018年6月至2022年12月期间确诊为UC且有≥1次UC全身治疗索赔(索引日期)的患者,此外在索引日期前连续注册≥6个月且在索引日期后连续注册≥12个月。如果患者在索引时年龄<18岁,或在索引前期间有过UC全身治疗索赔,确诊为克罗恩病或白塞病,或在索引前期间有结肠切除术记录,则排除该患者。感兴趣的结果是治疗模式、医疗资源利用(HCRU)和每人每月UC相关成本(PPPM)。进行了进一步的探索性分析,以了解传统疗法的实际治疗模式是否与指南建议最佳匹配。确定了传统疗法次优治疗的两种定义:长期使用皮质类固醇(即连续使用>90天)和皮质类固醇循环(即1年内有三个或更多≥30天的皮质类固醇疗程,疗程之间间隔≥60天)。
总体而言,共纳入15429例患者。最常观察到的一线治疗类别是5-氨基水杨酸单药治疗(75.0%);39.7%的患者出现治疗调整。在随访的1年内,患者平均(标准差)门诊就诊9.8次(6.8次),23.9%的患者报告有住院治疗。平均总PPPM成本为76374日元。在接受过≥1个皮质类固醇疗程的患者中,39.8%接受了传统疗法的次优治疗。接受传统疗法次优治疗的患者与未接受次优治疗的患者相比,HCRU和总成本更高。
日本UC患者将从能够降低成本、HCRU以及传统疗法次优治疗的治疗选择中获益。