Xiao Xia, Huang Pei, Xu Xiao-Ting
Department of Oncology, Wuxi No.2 People' s Hospital, Jiangnan University Medical Center, Wuxi, Jiangsu Province, China.
Department of Radiation Oncology, The First Affiliated Hospital of Soochow University, Suzhou, Jiangsu Province, China.
PLoS One. 2025 Jan 24;20(1):e0317995. doi: 10.1371/journal.pone.0317995. eCollection 2025.
The role of adjuvant radiotherapy in pancreatic cancer following radical surgery remains a subject of of controversy. This study aimed to more accurately screen pancreatic patients who benefit from adjuvant radiotherapy.
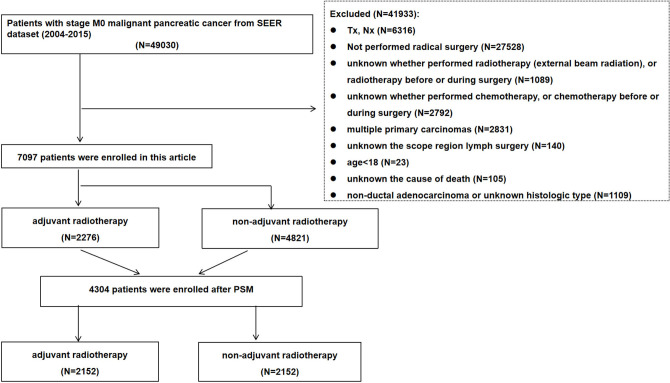
Clinicopathologic characteristics of patients with resectable pancreatic cancer were collected from the Surveillance, Epidemiology, and End Results (SEER) database (2004-2015). Univariate and multivariate analyses were applied to identify prognostic factors affecting patient survival. All the patients were divided into two groups, one receiving radiation and the other not. Selection bias were reduced by propensity-score matching (PSM). Kaplan-Meier analysis was used to estimate overall survival (OS) and cancer-specific survival (CSS) between the two groups.
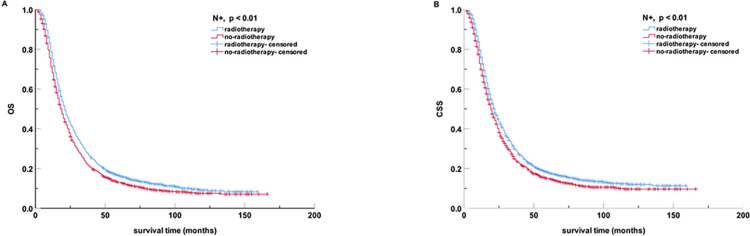
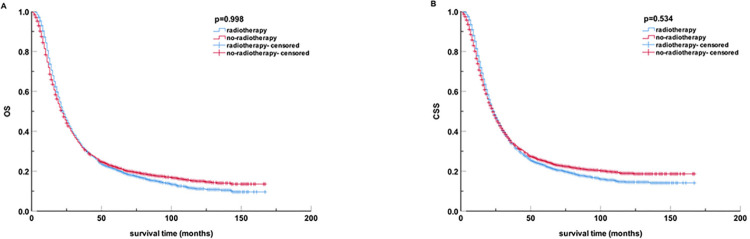
Within 7097 patients, 2276 received adjuvant radiotherapy (external beam radiation), and 4821 did not. Multivariate analysis revealed that race, age, median income, sex, year of diagnosis, American Joint Committee on Cancer (AJCC) T stage, N stage, scope region lymph surgery, chemotherapy, and radiotherapy were independent predictors for overall survival of all the patients (all p < 0.05). After PSM, a total of 4304 patients were included. There was no OS and CSS benefit of radiotherapy compared with no-radiotherapy (all p > 0.05). Among patients with N1 stage, the radiotherapy group exhibited a median overall survival (mOS) of 21 months (95% CI, 19.82 to 22.18), while the non-radiotherapy group showed a slightly lower mOS of 18 months (95% CI, 16.88 to 19.12). Similarly, in terms of median cancer-specific survival (mCSS), the radiotherapy group demonstrated a mCSS of 22 months (95% CI, 20.79 to 23.21), whereas the non-radiotherapy group had a slightly shorter mCSS of 19 months (95% CI, 17.81 to 20.19). Radiotherapy reduced the all-cause mortality rate and cancer-specific mortality rate among patients with the N1 stage and T4 stage (all p < 0.05). In contrast, the patients in the radiotherapy group with the N0 stage (mOS, 28 months versus 34 months; mCSS, 30 months versus 41months), or primary focus on the body and tail of the pancreas (mOS, 23 months versus 29 months; mCSS, 25 months versus 32 months), or T1 stage (mOS, 36 months versus 113 months; mCSS, 36 months versus 104 months) exhibited a higher all-cause mortality rate and cancer-specific mortality rate compared to those without radiotherapy (all p < 0.05). Subgroup analysis indicated N1 stage pancreatic cancer patients with T2-4 stage, primary focus on the head of the pancreas, young age of onset, and combination chemotherapy were in favor of the adjuvant radiotherapy group (all p < 0.05).
Our analysis demonstrates that adjuvant radiotherapy may be beneficial for N1 stage (N+) pancreatic cancer patients who have undergone up-front radical surgery with T2-4 stage, primary focus on the head of the pancreas, young age of onset, and receiving combination chemotherapy. However, radiotherapy needs to be used with caution in patients with T1 stage, N0 stage (N-), or primary focus on the body and tail of the pancreas. These findings may contribute to the development of personalized selection criteria for adjuvant radiotherapy in post-surgical pancreatic cancer patients.
辅助放疗在胰腺癌根治术后的作用仍存在争议。本研究旨在更准确地筛选出能从辅助放疗中获益的胰腺癌患者。
从监测、流行病学和最终结果(SEER)数据库(2004 - 2015年)收集可切除胰腺癌患者的临床病理特征。应用单因素和多因素分析来确定影响患者生存的预后因素。所有患者分为两组,一组接受放疗,另一组未接受放疗。通过倾向评分匹配(PSM)减少选择偏倚。采用Kaplan - Meier分析评估两组之间的总生存期(OS)和癌症特异性生存期(CSS)。
在7097例患者中,2276例接受了辅助放疗(外照射放疗),4821例未接受。多因素分析显示,种族、年龄、收入中位数、性别、诊断年份、美国癌症联合委员会(AJCC)T分期、N分期、区域淋巴结清扫范围、化疗和放疗是所有患者总生存期的独立预测因素(所有p < 0.05)。PSM后,共纳入4304例患者。与未放疗组相比,放疗组在OS和CSS方面无获益(所有p > 0.05)。在N1期患者中,放疗组的中位总生存期(mOS)为21个月(95%CI,19.82至22.18),而未放疗组的mOS略低,为18个月(95%CI,16.88至19.12)。同样,在中位癌症特异性生存期(mCSS)方面,放疗组为22个月(95%CI,20.79至23.21),而未放疗组略短,为19个月(95%CI,17.81至20.19)。放疗降低了N1期和T4期患者的全因死亡率和癌症特异性死亡率(所有p < 0.05)。相比之下,放疗组中N0期(mOS,28个月对34个月;mCSS,30个月对41个月)、或肿瘤原发灶位于胰体尾(mOS,23个月对29个月;mCSS,