Chen Ping, Wang Xiuqin, Mou Yun
Echocardiography and Vascular Ultrasound Center, The First Affiliated Hospital, Zhejiang University School of Medicine, 79 Qingchun Road, Hangzhou, 310003, China.
J Cardiothorac Surg. 2025 Jan 27;20(1):99. doi: 10.1186/s13019-024-03271-z.
Interventricular septal dissection is a critical disease characterized by the separation of the intraventricular septum into two layers, forming an intermediate layer with a cystic cavity that communicates with the root of the aorta or ventricle. It has low morbidity and high mortality rates.
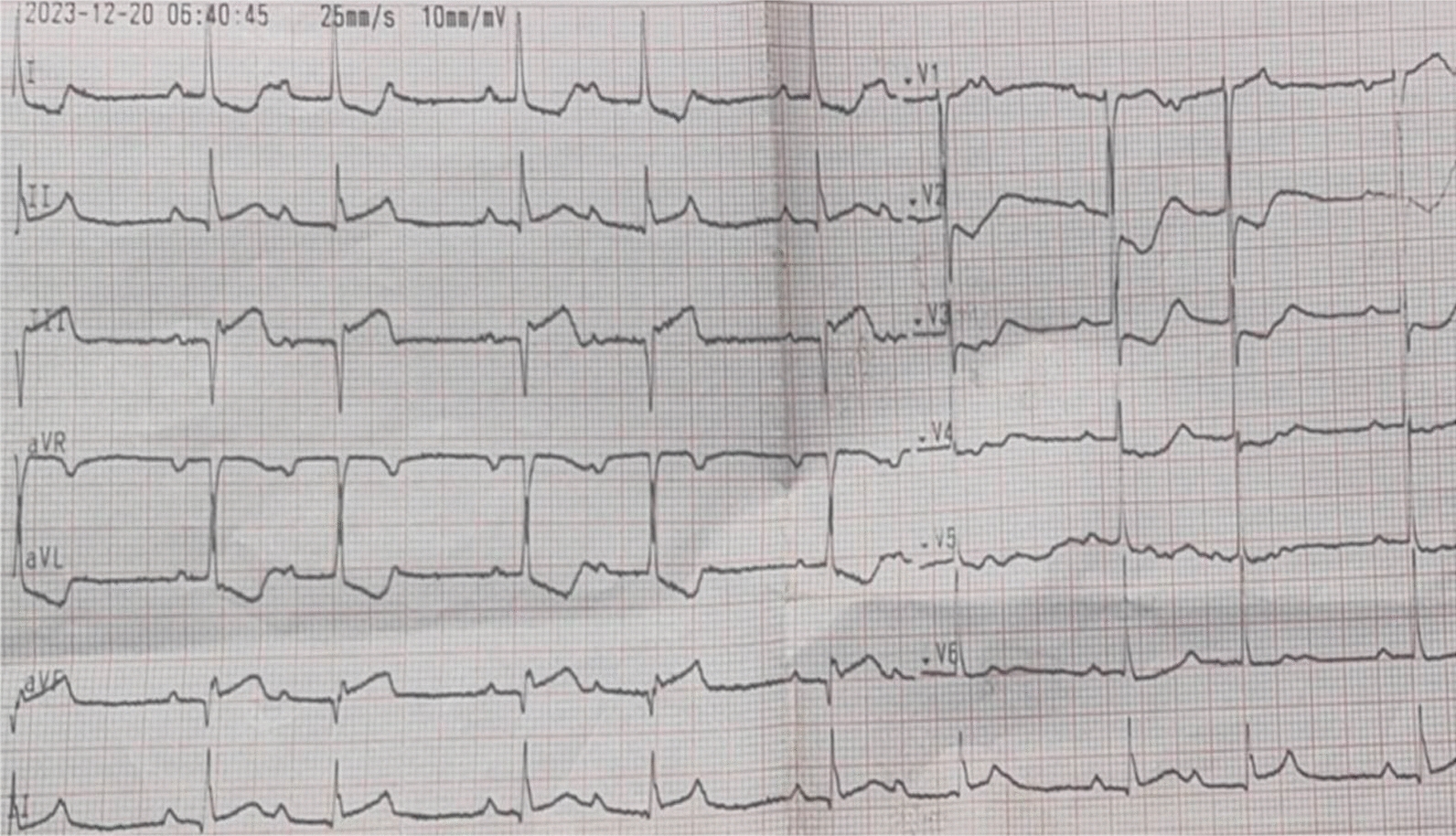
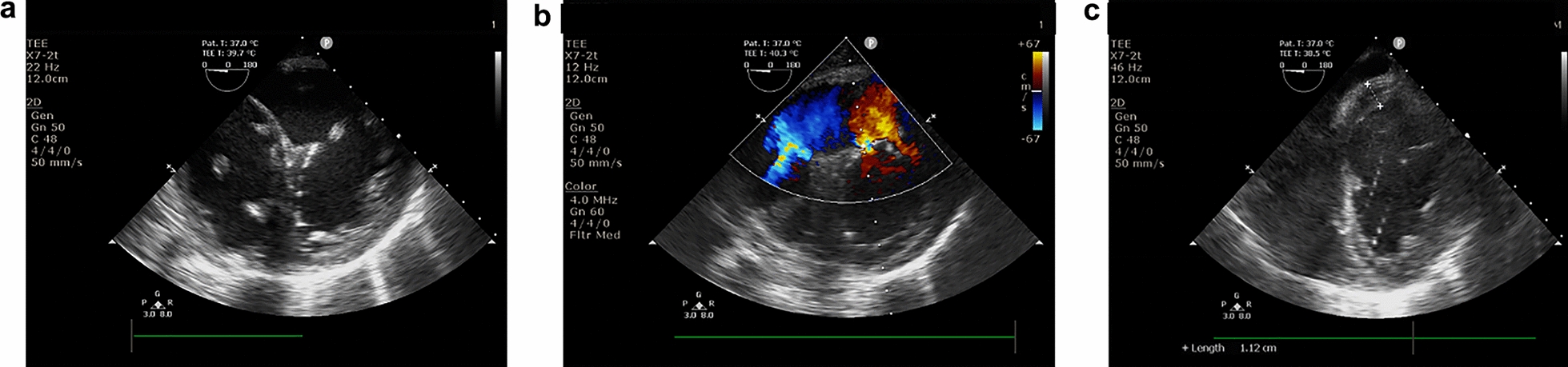
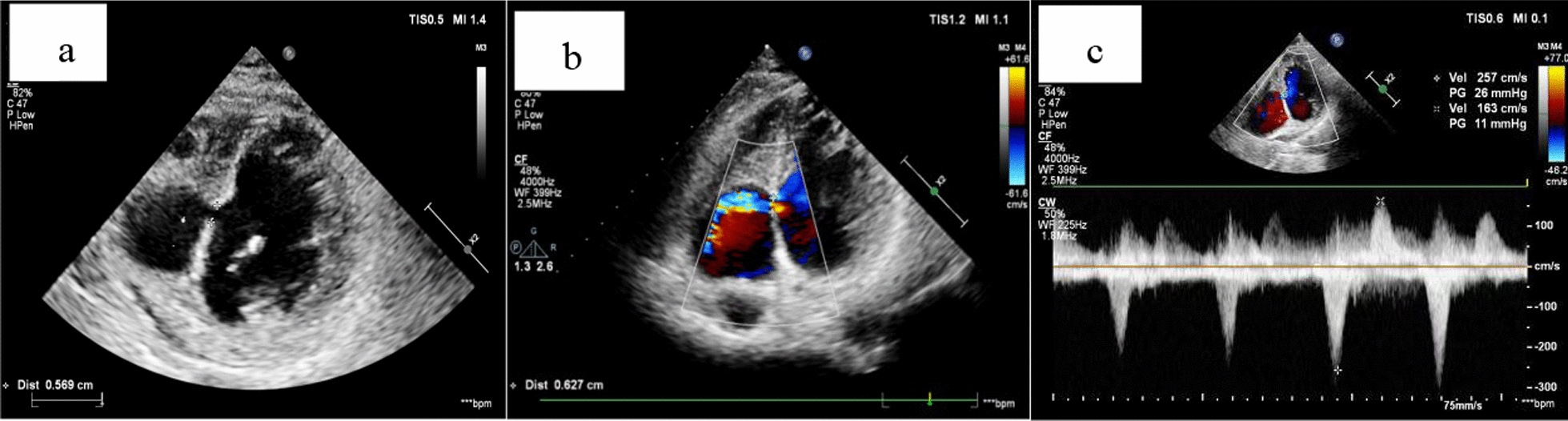
Case 1: A 58-year-old male with a history of hypertension and smoking presented to a local hospital due to chest tightness and pain for 4 days. Coronary angiography revealed diffuse lesions from the proximal to the middle segment of the left circumflex branch, with 80% stenosis at its most severe point, and complete occlusion of the proximal segment of the right coronary artery. A stent was implanted in the middle of the right coronary artery. Three months later, the patient was misdiagnosed with an aneurysm of the membranous ventricular septum with defect via echocardiography at the local hospital. After the implantation of a stent in the left circumflex branch, the patient came to our hospital for further diagnosis and treatment. The first ultrasound of our hospital misdiagnosed it as ventricular septal rupture, and a senior ultrasound doctor diagnosed the patient with interventricular septal dissection secondary to myocardial infarction. The patient underwent follow-up echocardiography every 1-2 months for 6 months. The patient remains asymptomatic with stable hemodynamics. The original treatment regimen and follow-up continues. Case 2: A 70-year-old male was admitted to a local hospital due to repeated chest distress for more than 20 years that worsened over several hours. Coronary angiography revealed complete occlusion of the right coronary artery. Cardiogenic shock occurred after percutaneous coronary intervention. The initial several echocardiography of the local hospital and our hospital misdiagnosed it as interventricular septal rupture secondary to myocardial infarction. The later echocardiography diagnosed it as interventricular septal dissection with rupture secondary to myocardial infarction. The patient underwent interventricular septal repair and mitral valvuloplasty after 25 days of medical treatment and died of multiple organ failure on the fourth day after the operation.
These two cases illustrate a complication of acute myocardial infarction and highlight the importance of echocardiography in its diagnosis. By exploring the etiology, pathogenesis, and key diagnostic points of IVSD, this study aims to provide valuable insights for clinical practice.
室间隔夹层是一种危急病症,其特征为室间隔分为两层,形成一个带有与主动脉根部或心室相通的囊腔的中间层。它发病率低但死亡率高。
病例1:一名58岁男性,有高血压和吸烟史,因胸闷、胸痛4天就诊于当地医院。冠状动脉造影显示左旋支近端至中段弥漫性病变,最严重处狭窄80%,右冠状动脉近端完全闭塞。在右冠状动脉中段植入了支架。3个月后,当地医院经超声心动图误诊为膜周部室间隔瘤伴缺损。左旋支植入支架后,患者来我院进一步诊治。我院首次超声误诊为室间隔破裂,一名资深超声医生诊断该患者为心肌梗死后室间隔夹层。患者每1 - 2个月接受一次超声心动图随访,共6个月。患者无症状,血流动力学稳定。继续原治疗方案及随访。病例2:一名70岁男性因反复胸闷20余年,数小时内加重入住当地医院。冠状动脉造影显示右冠状动脉完全闭塞。经皮冠状动脉介入治疗后发生心源性休克。当地医院和我院最初几次超声心动图误诊为心肌梗死后室间隔破裂。后来的超声心动图诊断为心肌梗死后室间隔夹层伴破裂。患者经25天药物治疗后行室间隔修补及二尖瓣成形术,术后第4天死于多器官功能衰竭。
这两个病例说明了急性心肌梗死的一种并发症,并强调了超声心动图在其诊断中的重要性。通过探讨室间隔夹层的病因、发病机制及关键诊断要点,本研究旨在为临床实践提供有价值的见解。