Chipman Amanda M, Luther James F, Guyette Francis X, Cotton Bryan A, Cannon Jeremy W, Schreiber Martin A, Moore Ernest E, Namias Nicholas, Minei Joseph P, Yazer Mark H, Vincent Laura, Cotton Abigail L, Agarwal Vikas, Brown Joshua B, Leeper Christine M, Neal Matthew D, Forsythe Raquel M, Wisniewski Stephen R, Sperry Jason L
From the Department of Surgery (A.M.C., L.V., A.L.C.), University of Pittsburgh; University of Pittsburgh School of Public Health (J.F.L., S.R.W.); Department of Emergency Medicine (F.X.G.), University of Pittsburgh, Pittsburgh, Pennsylvania; Department of Surgery (B.A.C.), University of Texas Health Science Center, Houston, Texas; Department of Surgery (J.W.C.), University of Pennsylvania, Philadelphia, Pennsylvania; Department of Surgery (M.A.S.), Oregon Health & Science University, Portland, Oregon; Department of Surgery (E.E.M.), Ernest E. Moore Shock Trauma Center at Denver Health, University of Colorado Health Sciences Center, Denver, Colorado; Department of Surgery (N.N.), University of Miami/Jackson Memorial Hospital, Miami, Florida; Department of Surgery (J.P.M.), University of Texas Southwestern Medical Center, Dallas, Texas; and Department of Pathology (M.H.Y.), Department of Radiology (V.A.), and Trauma and Transfusion Medicine Research Center, Department of Surgery (J.B.B., C.M.L., M.D.N., R.M.F., J.L.S.), University of Pittsburgh, Pittsburgh, Pennsylvania.
J Trauma Acute Care Surg. 2025 Mar 1;98(3):393-401. doi: 10.1097/TA.0000000000004507. Epub 2025 Jan 27.
Whole blood resuscitation is associated with survival benefits in observational cohort studies. The mechanisms responsible for outcome benefits have not been adequately determined. We sought to characterize the achievement of hemostasis across patients receiving early whole blood versus component resuscitation. We hypothesized that achieving hemostasis would be associated with outcome benefits and patients receiving whole blood would be more likely to achieve hemostasis.
We performed a post hoc retrospective secondary analysis of data from a recent prospective observational cohort study comparing early whole blood and component resuscitation in patients at risk of hemorrhagic shock. Achievement of hemostasis was defined by receiving a single unit of blood or less, including whole blood or red cells, in any 60-minute period, over the first 4 hours from the time of arrival. Time-to-event analysis with log-rank comparison and regression modeling were used to determine the independent benefits of achieving hemostasis and whether achieving hemostasis was associated with whole blood resuscitation.
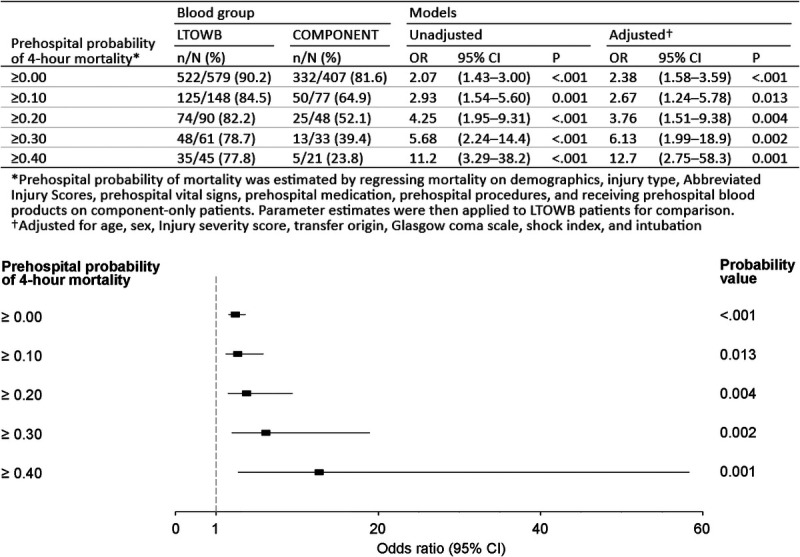
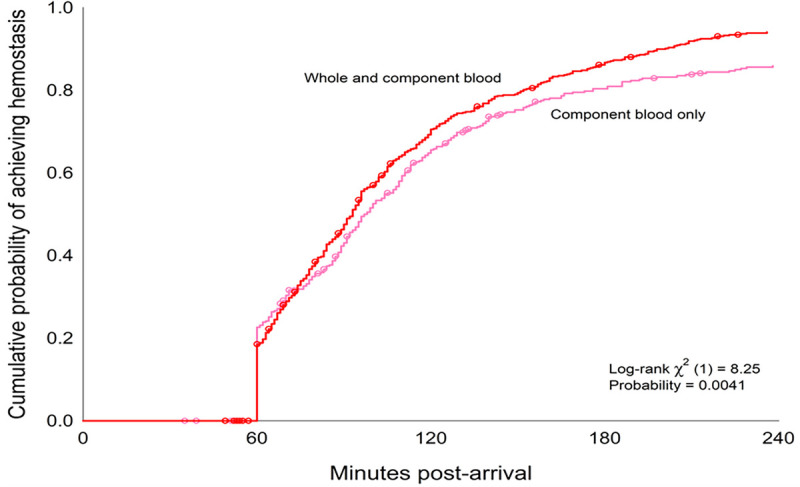
For the current analysis, 1,047 patients met the inclusion criteria for the study. When we compared patients who achieved hemostasis versus those who did not, achievement of hemostasis had significantly more hemostatic coagulation parameters, had lower transfusion requirements, and was independently associated with 4-hour, 24-hour and 28-day survival. Whole blood patients were significantly more likely to achieve hemostasis (88.9% vs. 81.1%, p < 0.001). Whole blood patients achieved hemostasis earlier (log-rank χ 2 = 8.2, p < 0.01) and were independently associated with over twofold greater odds of achieving hemostasis (odds ratio, 2.4; 95% confidence interval, 1.6-3.7; p < 0.001).
Achievement of hemostasis is associated with significant outcome benefits. Early whole blood resuscitation is associated with a greater independent odds of achieving hemostasis and at an earlier time point. Reaching a nadir transfusion rate early following injury represents a possible mechanism of whole blood resuscitation and its attributable outcome benefits.
Therapeutic/Care Management; Level III.
在观察性队列研究中,全血复苏与生存获益相关。导致预后获益的机制尚未得到充分确定。我们试图描述接受早期全血复苏与成分复苏的患者实现止血的情况。我们假设实现止血与预后获益相关,且接受全血复苏的患者更有可能实现止血。
我们对最近一项前瞻性观察性队列研究的数据进行了事后回顾性二次分析,该研究比较了出血性休克风险患者的早期全血复苏和成分复苏。止血的实现定义为从到达时间起的前4小时内,在任何60分钟时间段内接受单单位血液或更少,包括全血或红细胞。采用对数秩比较的生存时间分析和回归模型来确定实现止血的独立获益以及实现止血是否与全血复苏相关。
对于当前分析,1047例患者符合研究纳入标准。当我们比较实现止血的患者与未实现止血的患者时,实现止血的患者具有更多显著的止血凝血参数,输血需求更低,并且与4小时、24小时和28天生存率独立相关。全血复苏患者实现止血的可能性显著更高(88.9%对81.1%,p<0.001)。全血复苏患者更早实现止血(对数秩χ2 = 8.2,p<0.01),并且与实现止血的几率高出两倍以上独立相关(优势比,2.4;95%置信区间,1.6 - 3.7;p<0.001)。
实现止血与显著的预后获益相关。早期全血复苏与更早实现止血的更大独立几率相关。受伤后尽早达到最低输血率代表了全血复苏及其可归因的预后获益的一种可能机制。
治疗/护理管理;三级。