Orgun Doruk, Bay Caroline C, Carbullido Kristine M, Wieland Aaron M, Michelotti Brett F, Poore Samuel O
Division of Plastic and Reconstructive Surgery, Department of Surgery, University of Wisconsin School of Medicine and Public Health, Madison, Wisconsin, U.S.A.
Department of Plastic and Reconstructive Surgery, The Jikei University School of Medicine, Tokyo, Japan.
Laryngoscope. 2025 Jul;135(7):2342-2352. doi: 10.1002/lary.32008. Epub 2025 Jan 27.
To investigate the consistency of associations between modified frailty index-5 (mFI-5) and postoperative adverse outcomes in head and neck cancer (HNC) reconstruction.
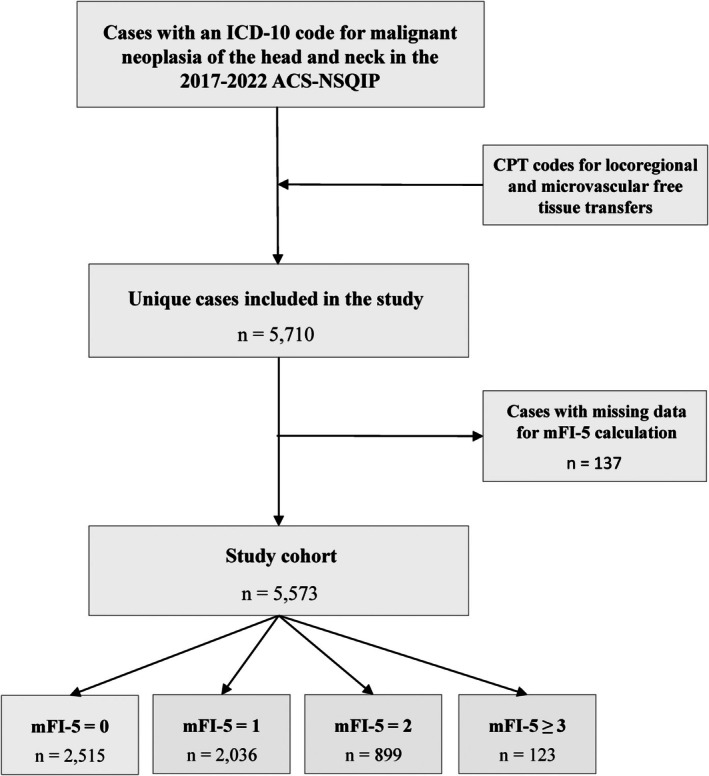
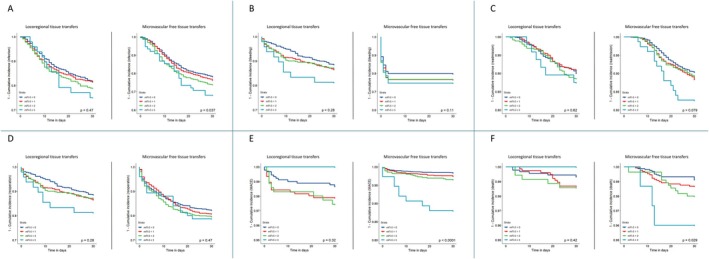
American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database from 2017 to 2022 was utilized to identify HNC patients undergoing locoregional or microvascular free tissue transfers. Kaplan-Meier estimates and multivariable Cox regression analyses were utilized to compare risk of infections, bleeding, readmissions, reoperations, major adverse cardiovascular events (MACE), and mortality within the first postoperative month for each mFI-5 score with mFI-5 = 0 as reference. Further analyses investigated associations between individual mFI-5 components and the outcomes of interest.
We included 5,573 patients (median age: 64; 31.5% female), 63% (n = 3,519) of whom underwent microvascular free tissue transfers. Unadjusted univariate analyses associated higher mFI-5 scores with longer hospital stays. In locoregional tissue transfers, adjusted hazard ratios (aHRs) for reoperation were 1.37 (p = 0.03) for mFI-5 = 1 and 2.19 (p = 0.03) for mFI-5 ≥ 3. In microvascular free tissue transfers, aHRs for MACE were 1.93 (p = 0.04) for mFI-5 = 2 and 6.53 (p < 0.001) for mFI-5 ≥ 3, while aHRs for mortality was 3.88 (p = 0.04) for mFI-5 ≥ 3. No associations were observed between increasing mFI-5 scores and increased relative risk of infection, bleeding, or readmission. Individual component analysis associated congestive heart failure with aHRs of 3.92 (1.84-8.35; p < 0.001) for MACE and 5.30 (2.03-13.88; p < 0.001) for mortality. Additionally, COPD was associated with an aHR of 1.39 (1.16-1.67; p < 0.001) for infections.
The associations of higher mFI-5 scores with postoperative adverse outcomes following oncoplastic head and neck reconstruction were inconsistent and possibly driven by individual effects of its components.
3 Laryngoscope, 135:2342-2352, 2025.
研究改良脆弱指数-5(mFI-5)与头颈癌(HNC)重建术后不良结局之间关联的一致性。
利用美国外科医师学会国家外科质量改进计划(ACS-NSQIP)2017年至2022年的数据库,识别接受局部或微血管游离组织移植的HNC患者。采用Kaplan-Meier估计法和多变量Cox回归分析,以mFI-5 = 0为参照,比较每个mFI-5评分在术后第一个月内发生感染、出血、再次入院、再次手术、主要不良心血管事件(MACE)和死亡的风险。进一步分析调查了mFI-5各个组成部分与感兴趣结局之间的关联。
我们纳入了5573例患者(中位年龄:64岁;31.5%为女性),其中63%(n = 3519)接受了微血管游离组织移植。未经调整的单变量分析显示,mFI-5评分越高,住院时间越长。在局部组织移植中,mFI-5 = 1时再次手术的调整后风险比(aHRs)为1.37(p = 0.03),mFI-5≥3时为2.19(p = 0.03)。在微血管游离组织移植中,mFI-5 = 2时MACE的aHRs为1.93(p = 0.04),mFI-5≥3时为6.53(p < 0.001),而mFI-5≥3时死亡的aHRs为3.88(p = 0.04)。未观察到mFI-5评分增加与感染、出血或再次入院相对风险增加之间存在关联。个体成分分析显示,充血性心力衰竭与MACE的aHRs为3.92(1.84 - 8.35;p < 0.001),与死亡的aHRs为5.30(2.03 - 13.88;p < 0.001)。此外,慢性阻塞性肺疾病(COPD)与感染的aHR为1.39(1.16 - 1.67;p < 0.001)。
mFI-5评分较高与肿瘤整形头颈重建术后不良结局之间的关联不一致,可能是由其各个组成部分的个体效应驱动的。
3《喉镜》,135:2342 - 2352,2025年。