Paróczai Dóra, Bikov András, Blidaru Andreea, Bobu Emanuel, Lascu Ana, Mot Cristian Ion, Mihaicuta Stefan, Frent Stefan
Department of Medical Microbiology, University of Szeged, Szeged, Hungary.
Albert Szent-Györgyi Health Center, Pulmonology Clinic, University of Szeged, Deszk, Hungary.
Front Cell Infect Microbiol. 2025 Jan 16;14:1496176. doi: 10.3389/fcimb.2024.1496176. eCollection 2024.
Drug repurposing has become a widely adopted strategy to minimise research time, costs, and associated risks. Combinations of protease inhibitors such as lopinavir and darunavir with ritonavir have been repurposed as treatments for COVID-19. Although lopinavir-ritonavir (LPV/r) and darunavir-ritonavir (DRV/r) have shown efficacy against COVID-19, the results in human studies have been inconsistent. Therefore, our objective was to compare the efficacy of LPV/r and DRV/r in COVID-19 patients admitted to a tertiary centre in Romania.
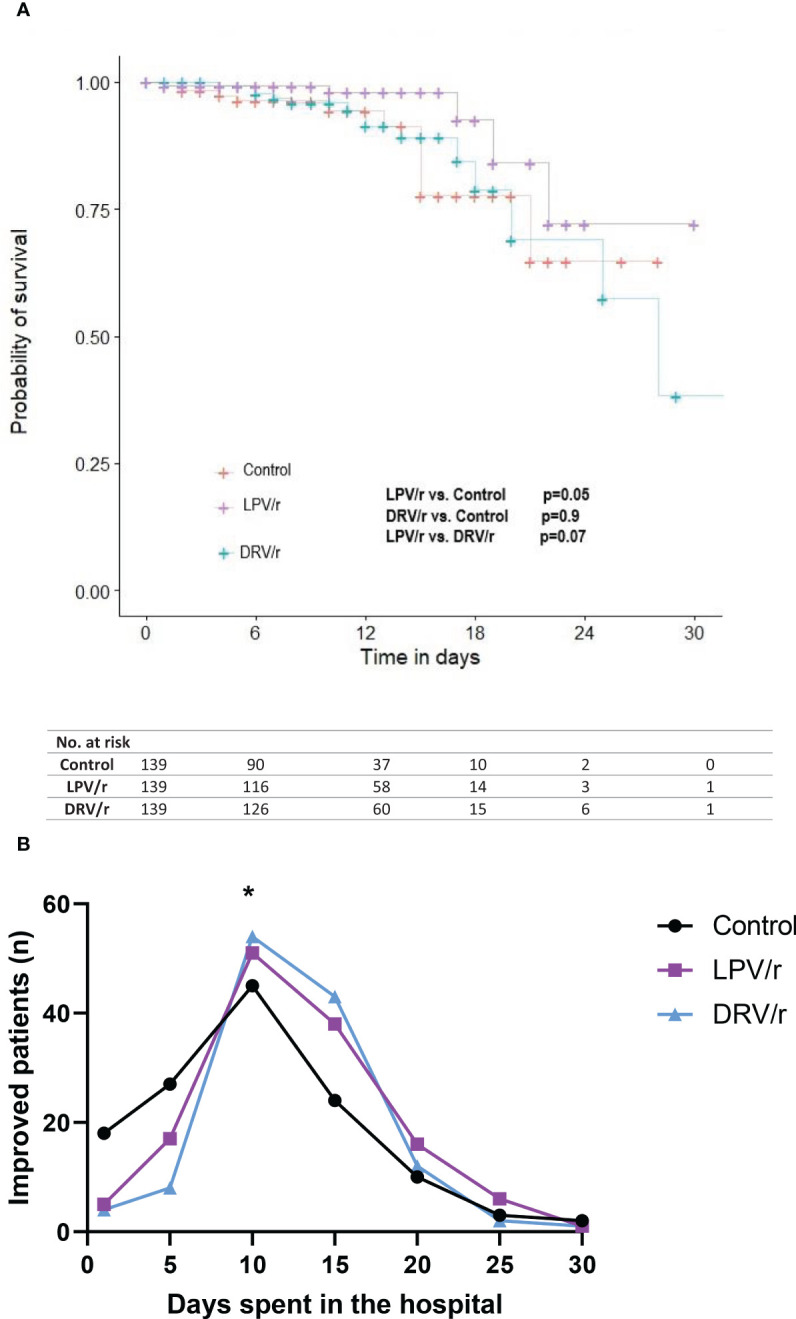
A clinical dataset from 417 hospitalised patients was analysed. Patients were assigned to the LPV/r, DRV/r, or control (standard-of-care) group based on clinical decisions made by the attending infectious disease specialists, aligned with national treatment protocols. Kaplan-Meier and Cox proportional hazards regression analyses were conducted to compare in-hospital mortality and to identify factors associated with clinical improvement or fatal outcomes.
By day 10, more patients showed improvement with LPV/r and DRV/r (p=0.03 and 0.01, respectively), but only LPV/r was associated with improved survival compared to the control group (p=0.05). Factors associated with mortality included male gender (HR: 3.63, p=0.02), diabetes (HR: 2.49, p=0.03), oxygen saturation below 90% at admission (HR: 5.23, p<0.01), high blood glucose levels (HR: 3.68, p=0.01), age (HR: 1.04, p=0.02), and more than 25% lesion extension on chest CT scan (HR: 2.28, p=0.03).
LPV/r, but not DRV/r, showed a survival benefit in patients hospitalised with COVID-19, but these findings deserve further investigation in a randomised clinical trial.
药物重新定位已成为一种广泛采用的策略,以尽量减少研究时间、成本和相关风险。洛匹那韦和达芦那韦等蛋白酶抑制剂与利托那韦的组合已被重新定位用于治疗新冠病毒病(COVID-19)。尽管洛匹那韦-利托那韦(LPV/r)和达芦那韦-利托那韦(DRV/r)已显示出对COVID-19的疗效,但人体研究结果并不一致。因此,我们的目标是比较LPV/r和DRV/r在罗马尼亚一家三级中心收治的COVID-19患者中的疗效。
分析了417例住院患者的临床数据集。根据主治传染病专家根据国家治疗方案做出的临床决策,将患者分为LPV/r组、DRV/r组或对照组(标准治疗组)。进行了Kaplan-Meier分析和Cox比例风险回归分析,以比较住院死亡率,并确定与临床改善或致命结局相关的因素。
到第10天,更多使用LPV/r和DRV/r的患者病情有所改善(分别为p = 0.03和0.01),但与对照组相比,只有LPV/r与生存率提高相关(p = 0.05)。与死亡率相关的因素包括男性(风险比:3.63,p = 0.02)、糖尿病(风险比:2.49,p = 0.03)、入院时血氧饱和度低于90%(风险比:5.23,p<0.01)、高血糖水平(风险比:3.68,p = 0.01)、年龄(风险比:1.04,p = 0.02)以及胸部CT扫描显示病变扩展超过25%(风险比:2.28,p = 0.03)。
LPV/r而非DRV/r在COVID-19住院患者中显示出生存获益,但这些发现值得在随机临床试验中进一步研究。