Rodriguez Patricia J, Zhang Vincent, Gratzl Samuel, Do Duy, Goodwin Cartwright Brianna, Baker Charlotte, Gluckman Ty J, Stucky Nicholas, Emanuel Ezekiel J
Truveta Inc, Bellevue, Washington.
Healthcare Transformation Institute, Department of Medical Ethics and Health Policy, Perelman School of Medicine at the University of Pennsylvania, Philadelphia.
JAMA Netw Open. 2025 Jan 2;8(1):e2457349. doi: 10.1001/jamanetworkopen.2024.57349.
Adherence to glucagon-like peptide-1 receptor agonists (GLP-1 RAs) is important for their effectiveness. Discontinuation and reinitiation patterns are not well understood.
To describe rates of and factors associated with discontinuation and subsequent reinitiation of GLP-1 RAs among adults with overweight or obesity.
DESIGN, SETTING, AND PARTICIPANTS: In this retrospective cohort study, 125 474 adults with overweight or obesity newly initiated treatment with a dual-labeled GLP-1 RA (liraglutide, semaglutide, or tirzepatide) between January 1, 2018, and December 31, 2023, with a baseline body mass index of 27 or more, an available weight measurement within 60 days before initiation, and regular care in the year before initiation were identified using electronic health record data from a collective of US health care systems. Patients were followed up for up to 2 years to assess discontinuation and for 2 additional years to assess reinitiation.
Patients were stratified by presence of type 2 diabetes at baseline.
Proportions of patients discontinuing and reinitiating GLP-1 RA were estimated from Kaplan-Meier models. Associations of sociodemographic characteristics, health factors, weight changes, and gastrointestinal adverse events with discontinuation and reinitiation outcomes were modeled using time-varying Cox proportional hazards regression models. All analyses were conducted separately for patients with and patients without type 2 diabetes.
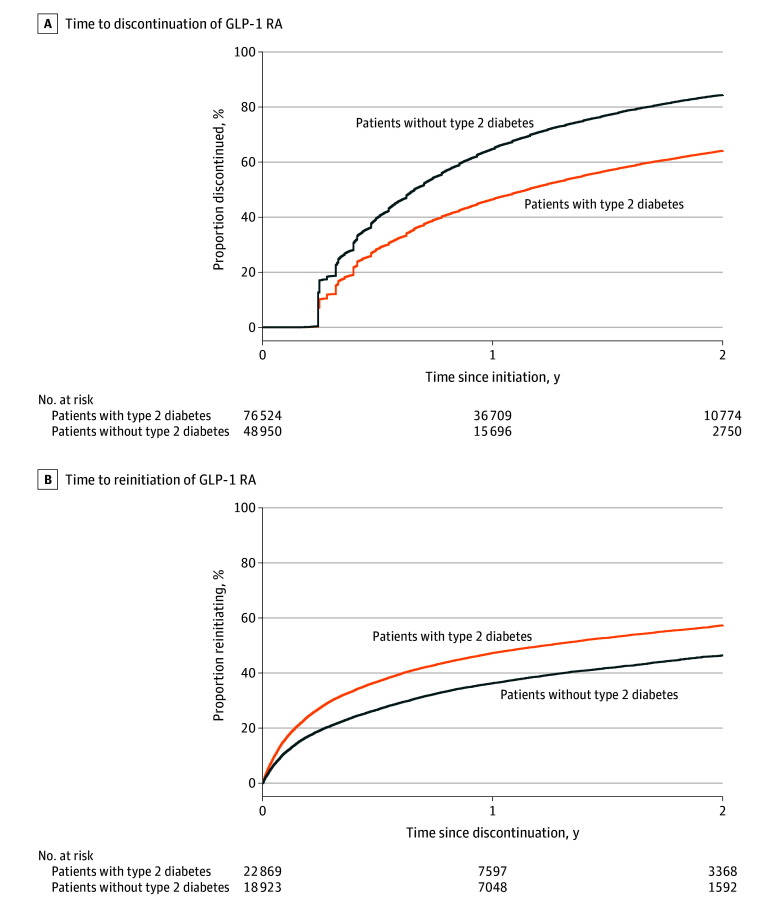
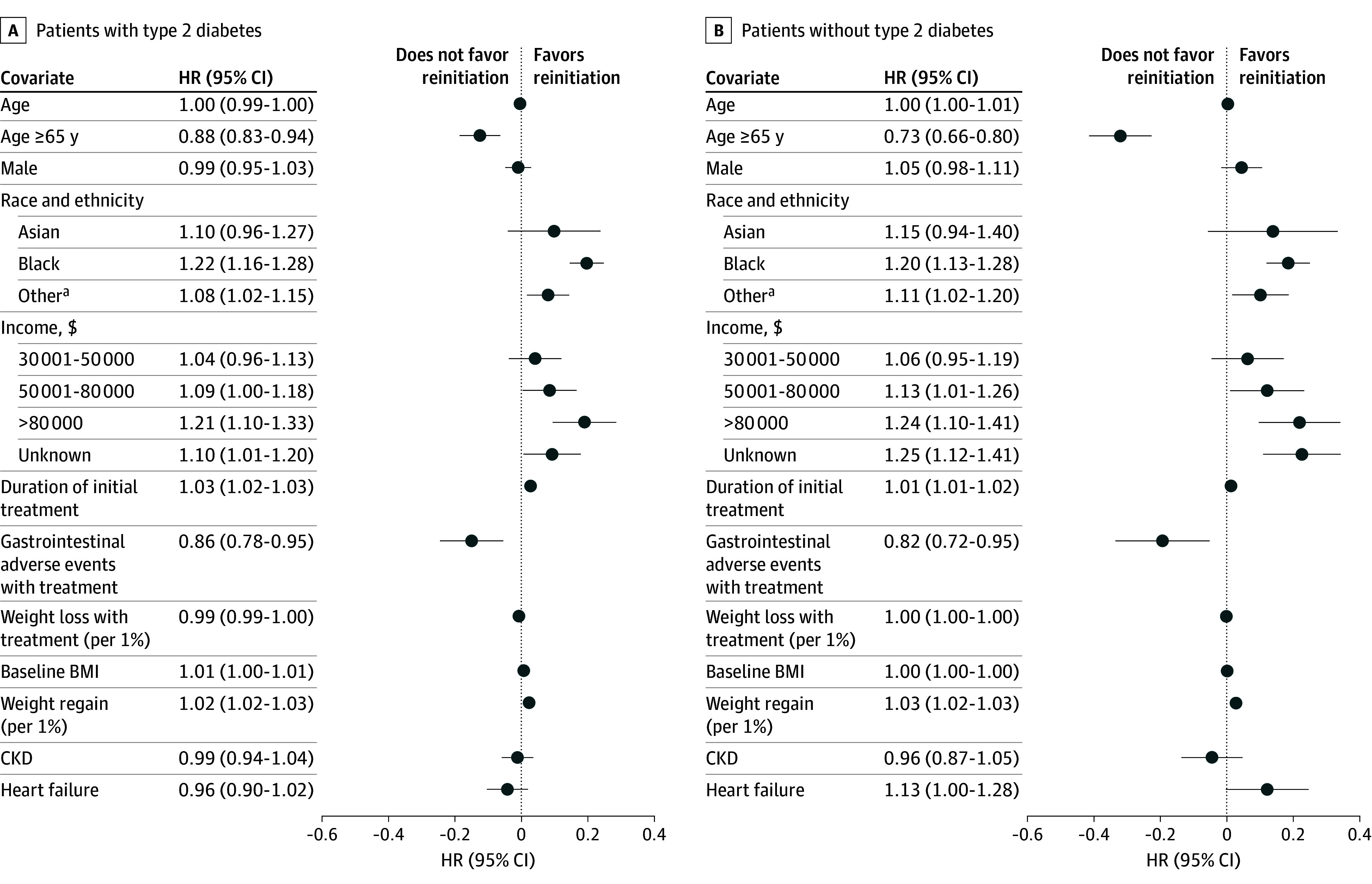
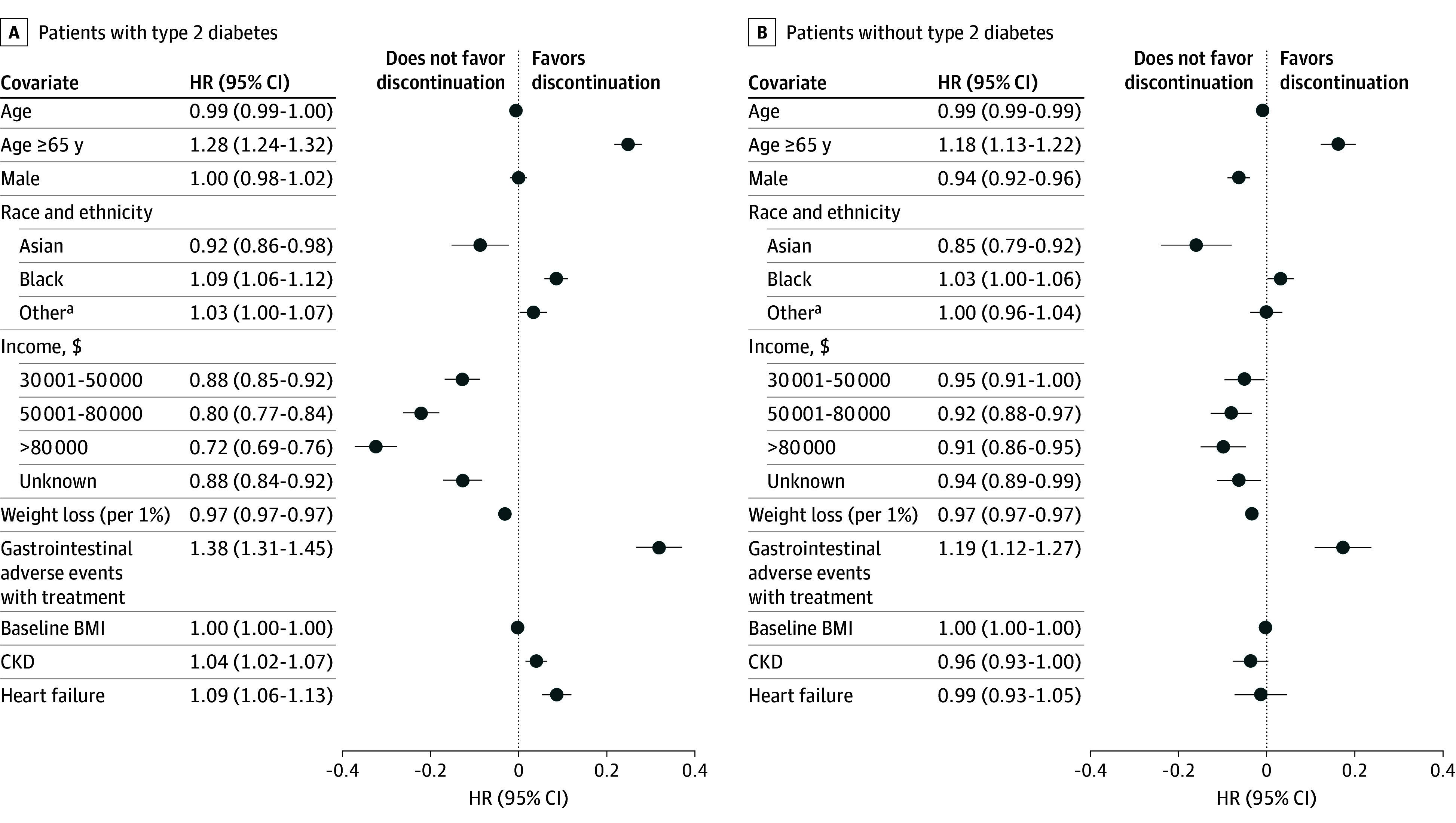
In this cohort study of 125 474 adults (mean [SD] age, 54.4 [13.1] years; 82 063 women [65.4%]), 76 524 (61.0%) had type 2 diabetes. One-year discontinuation was significantly higher for patients without type 2 diabetes (64.8% [95% CI, 64.4%-65.2%]) compared with those with type 2 diabetes (46.5% [95% CI, 46.2%-46.9%]). Higher weight loss (1% reduction in weight from baseline was associated with a 3.1% [95% CI, 2.9%-3.2%] lower hazard of discontinuation for patients with type 2 diabetes and a 3.3% [95% CI, 3.2%-3.5%] lower hazard of discontinuation for patients without type 2 diabetes) and higher income (type 2 diabetes only; >$80 000: hazard ratio [HR], 0.72 [95% CI, 0.69-0.76]) were significantly associated with lower rates of discontinuation, while moderate or severe incident gastrointestinal adverse events were associated with a higher hazard of discontinuation (with type 2 diabetes: HR, 1.38 [95% CI, 1.31-1.45]; without type 2 diabetes: HR, 1.19 [95% CI, 1.12-1.27]). Of 41 792 patients who discontinued and had a discontinuation weight measurement available, 1-year reinitiation was lower for those without type 2 diabetes (36.3% [95% CI, 35.6%-37.0%]) compared with those with type 2 diabetes (47.3% [95% CI, 46.6%-48.0%]). Weight regain of 1% from discontinuation was significantly associated with increased hazards of reinitiation of 2.3% (95% CI, 1.9%-2.8%) for patients with type 2 diabetes and 2.8% (95% CI, 2.4%-3.2%) for patients without type 2 diabetes.
In this cohort study, most patients with overweight or obesity discontinued GLP-1 RA therapy within 1 year, but those without type 2 diabetes had higher discontinuation rates and lower reinitiation rates. Inequities in access and adherence to effective treatments have the potential to exacerbate disparities in obesity.
坚持使用胰高血糖素样肽-1受体激动剂(GLP-1 RA)对于其有效性至关重要。停药和重新开始用药的模式尚未得到充分了解。
描述超重或肥胖成年人中GLP-1 RA停药及随后重新开始用药的发生率和相关因素。
设计、设置和参与者:在这项回顾性队列研究中,利用美国医疗保健系统集体的电子健康记录数据,识别出125474名超重或肥胖成年人,他们在2018年1月1日至2023年12月31日期间新开始使用双标签GLP-1 RA(利拉鲁肽、司美格鲁肽或替尔泊肽)进行治疗,基线体重指数为27或更高,在开始治疗前60天内有可用的体重测量值,且在开始治疗前一年接受常规护理。对患者进行长达2年的随访以评估停药情况,并再额外随访2年以评估重新开始用药情况。
患者按基线时是否存在2型糖尿病进行分层。
通过Kaplan-Meier模型估计停药和重新开始使用GLP-1 RA的患者比例。使用时变Cox比例风险回归模型对社会人口学特征、健康因素、体重变化和胃肠道不良事件与停药和重新开始用药结局之间的关联进行建模。所有分析分别针对有和没有2型糖尿病的患者进行。
在这项对125474名成年人(平均[标准差]年龄为54.4[13.1]岁;82063名女性[65.4%])的队列研究中,76524名(61.0%)患有2型糖尿病。与患有2型糖尿病的患者(46.5%[95%置信区间,46.2%-46.9%])相比,没有2型糖尿病的患者1年停药率显著更高(64.8%[95%置信区间,64.4%-65.2%])。体重减轻较多(与基线相比体重降低1%与2型糖尿病患者停药风险降低3.1%[95%置信区间,2.9%-3.2%]以及没有2型糖尿病的患者停药风险降低3.3%[95%置信区间,3.2%-3.5%]相关)和收入较高(仅针对2型糖尿病患者;>80000美元:风险比[HR],0.72[95%置信区间,0.69-0.76])与较低的停药率显著相关,而中度或重度新发胃肠道不良事件与较高的停药风险相关(患有2型糖尿病:HR,1.38[95%置信区间,1.31-1.45];没有2型糖尿病:HR,1.19[95%置信区间,1.12-1.27])。在41792名停药且有停药时体重测量值的患者中,没有2型糖尿病的患者1年重新开始用药率(36.3%[95%置信区间,35.6%-37.0%])低于患有2型糖尿病的患者(47.3%[95%置信区间,46.6%-48.0%])。与停药时相比体重增加1%与2型糖尿病患者重新开始用药风险增加2.3%(95%置信区间,1.9%-2.8%)以及没有2型糖尿病的患者重新开始用药风险增加2.8%(95%置信区间,2.4%-3.2%)显著相关。
在这项队列研究中,大多数超重或肥胖患者在1年内停用了GLP-1 RA治疗,但没有2型糖尿病的患者停药率更高且重新开始用药率更低。有效治疗的可及性和依从性方面的不公平可能会加剧肥胖方面的差异。