Foss Alexander J E, Almeida David, Cheung Chui Ming Gemmy, Ogura Yuichiro, de Cock Eduard, Empeslidis Theo
Department of Ophthalmology, Nottingham University Hospitals NHS Trust, Nottingham, UK.
Vitreoretinal Diseases and Surgery, Erie Retinal Surgery, Erie, PA, USA.
Ophthalmol Ther. 2025 Mar;14(3):489-514. doi: 10.1007/s40123-025-01093-3. Epub 2025 Feb 4.
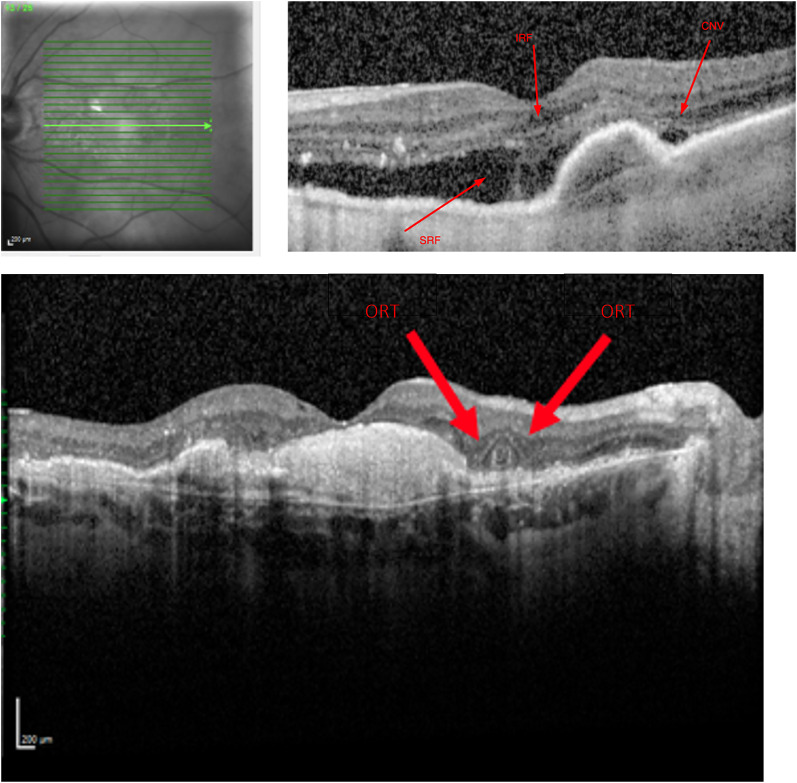
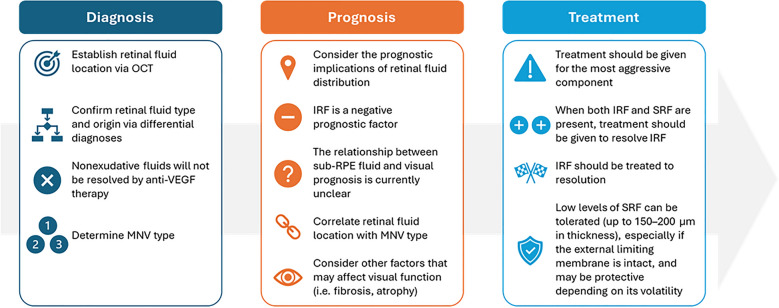
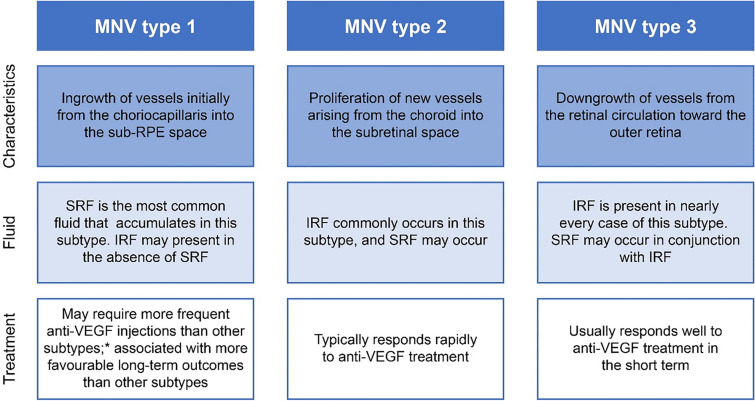
Neovascular age-related macular degeneration (nAMD) is associated with considerable quality of life and economic burden. nAMD is characterized by pathological neovascularization, leading to the accumulation of retinal fluid. Intraretinal fluid (IRF) is a major contributor to vision loss and may predict response to treatment. In contrast, the role of subretinal fluid (SRF) is less clear. Nevertheless, complete resolution of retinal fluid accumulation is often stated to be a key goal of therapy for nAMD, even though some eyes may never achieve a fluid-free macula despite regular anti-vascular endothelial growth factor treatment. In this article, we review the current literature regarding the role of retinal fluid in nAMD disease outcomes and assess whether and when it may be beneficial to leave retinal fluid untreated. In this context, we highlight the importance of correctly identifying retinal fluid types in nAMD and avoiding confusion with other optical coherence tomography signs that may respond differently to therapy, such as subretinal pseudocysts. Current evidence shows that IRF is associated with poor outcomes and an increased risk of developing atrophy and fibrosis; resolution of this retinal fluid type should remain a treatment target. However, the literature around SRF indicates that low levels of this fluid type, potentially up to 150-200 µm in thickness, may be tolerated with minimal impact on vision, and that SRF could be protective against the development and progression of macular atrophy and fibrosis. Although mild SRF may be protective in nAMD, cause and effect between SRF and reduced or slowed atrophy has not yet been proven and requires further research. Treatment should be given for the most aggressive component; when both IRF and SRF are present, treatment should be given for IRF.
新生血管性年龄相关性黄斑变性(nAMD)与相当大的生活质量和经济负担相关。nAMD的特征是病理性新生血管形成,导致视网膜液体积聚。视网膜内液(IRF)是导致视力丧失的主要因素,并且可能预测治疗反应。相比之下,视网膜下液(SRF)的作用尚不清楚。然而,尽管一些眼睛在接受常规抗血管内皮生长因子治疗后可能永远无法实现黄斑无液,但视网膜液体积聚的完全消退通常被认为是nAMD治疗的关键目标。在本文中,我们回顾了当前关于视网膜液在nAMD疾病预后中的作用的文献,并评估不治疗视网膜液是否以及何时可能有益。在此背景下,我们强调了在nAMD中正确识别视网膜液类型以及避免与其他光学相干断层扫描征象混淆的重要性,这些征象对治疗的反应可能不同,例如视网膜下假性囊肿。目前的证据表明,IRF与不良预后以及发生萎缩和纤维化的风险增加相关;这种视网膜液类型的消退应仍然是治疗目标。然而,关于SRF的文献表明,这种液体积聚水平较低(厚度可能高达150 - 200 µm)时,可能对视力影响最小而被耐受,并且SRF可能对黄斑萎缩和纤维化的发生和进展具有保护作用。尽管轻度SRF在nAMD中可能具有保护作用,但SRF与萎缩减轻或减缓之间的因果关系尚未得到证实,需要进一步研究。应针对最具侵袭性的成分进行治疗;当同时存在IRF和SRF时,应针对IRF进行治疗。