Barbero Manuel, Burgos Stefania, Roca Ignacio, Navarro Lucia, Cairo Fernando
Liver Transplant Unit, Hospital El Cruce de Florencio Varela, Buenos Aires, Argentina.
Medicine (Baltimore). 2025 Feb 7;104(6):e41378. doi: 10.1097/MD.0000000000041378.
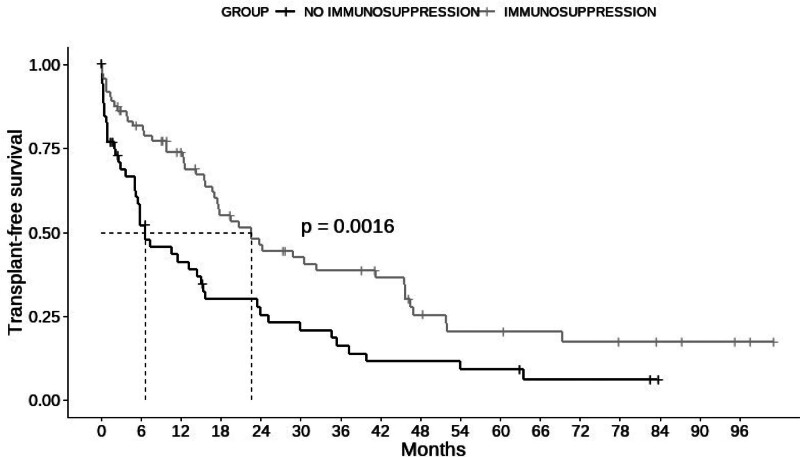
Immunosuppressive therapy in decompensated cirrhotic patients with an indication for liver transplantation (LT) is controversial. This study aims to evaluate transplant-free survival rates in patients diagnosed with decompensated autoimmune hepatitis (AIH) with and without immunosuppressants (IS) treatment, and to identify predictors of mortality or LT. We retrospectively analyzed LT-evaluated consecutive patients with decompensated AIH at a single center, between 2013 and 2021. Patients were categorized into IS (IS Group) and non-IS (No IS Group). Survival curves for the 2 groups were evaluated using the Kaplan-Meier method, and differences were compared using the Log-rank test. Multiple regression analysis was conducted using Cox test. A total of 125 consecutive patients (mean age: 36.4 years; 81.6% female) were evaluated. The median transplant-free survival in the IS Group (72/125) were 22.6 months vs 6.57 months in the No IS Group (53/125) (P = .002). Cox-regression analysis revealed associations between moderate/severe ascites (hazard ratio [HR] = 2.37, 95% CI = 1.48-3.80, P = <.001) and MELD-Na (HR = 1.12, 95% CI = 1.08-1.16, P = <.001) with transplantation or death, while immunosuppression treatment acted protectively (HR = 0.55, 95% CI = 0.86-0.85, P = .008). Analyzing patients with MELD >22 (27/125) showed a loss of IS protective effect (OR = 0.45, 95% CI = 0.17-1.20, P = .11), and the presence of moderate/severe ascites increased the risk of death/LT (HR = 5.86, 95% CI = 1.26-27.2, P = .02). Autoimmune decompensated cirrhosis is associated with high overall mortality, and IS improves the transplant-free survival rate. In patients with MELD-Na >22, treatment ceases to be beneficial, especially if they have moderate/severe ascites. These patients, if receiving immunosuppression, may be disadvantaged in the possibility of accessing LT.
对于有肝移植(LT)指征的失代偿期肝硬化患者,免疫抑制治疗存在争议。本研究旨在评估诊断为失代偿性自身免疫性肝炎(AIH)的患者在接受和未接受免疫抑制剂(IS)治疗情况下的无移植生存率,并确定死亡率或肝移植的预测因素。我们回顾性分析了2013年至2021年间在单一中心接受肝移植评估的连续性失代偿性AIH患者。患者被分为IS组(IS组)和非IS组(非IS组)。使用Kaplan-Meier方法评估两组的生存曲线,并使用对数秩检验比较差异。使用Cox检验进行多因素回归分析。共评估了125例连续性患者(平均年龄:36.4岁;81.6%为女性)。IS组(72/125)的无移植生存中位数为22.6个月,而非IS组(53/125)为6.57个月(P = 0.002)。Cox回归分析显示,中/重度腹水(风险比[HR]=2.37,95%置信区间[CI]=1.48 - 3.80,P = <0.001)和MELD-Na(HR = 1.12,95% CI = 1.08 - 1.16,P = <0.001)与移植或死亡相关,而免疫抑制治疗具有保护作用(HR = 0.55,95% CI = 0.86 - 0.85,P = 0.008)。对MELD>22的患者(27/125)进行分析显示,IS的保护作用丧失(比值比[OR]=0.45,95% CI = 0.17 - 1.20,P = 0.11),且中/重度腹水会增加死亡/肝移植风险(HR = 5.86,95% CI = 1.26 - 27.2,P = 0.02)。自身免疫性失代偿性肝硬化与高总体死亡率相关,IS可提高无移植生存率。在MELD-Na>22的患者中,治疗不再有益,尤其是如果他们有中/重度腹水。这些患者如果接受免疫抑制治疗,在获得肝移植的可能性方面可能处于不利地位。