Hubertus Vanessa, Wagner Arthur, Karbe Arian, Leonhardt Leon-Gordian, Kunze Beate, Borchert Susanne, Kilinc Fatma, Mariño Michelle, Nissimov Nitzan, Buhre Charlotte, Czabanka Marcus, Dreimann Marc, Eicker Sven O, Viezens Lennart, Meyer Hanno S, Vajkoczy Peter, Meyer Bernhard, Onken Julia S
Department of Neurosurgery, Charité - Universitätsmedizin Berlin, corporate member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Berlin, Germany.
Department of Neurosurgery, School of Medicine, Klinikum Rechts der Isar, Technical University of Munich, Munich, Germany.
Brain Spine. 2025 Jan 31;5:104198. doi: 10.1016/j.bas.2025.104198. eCollection 2025.
Spinal metastases at the thoracolumbar junction (TLJ) pose a significant risk for spinal instability and necessitate special considerations regarding surgical management. Longer patient survival due to improved oncologic therapies may justify extensive instrumented surgery.
The aim of this study was to analyze the standard of care in a large multicentric cohort of patients with TLJ metastases regarding surgical decision-making, management, and associated morbidity.
Patients with surgically treated spinal metastases at the TLJ between 2010 and 2022 were enrolled at five academic tertiary spine centers. Epidemiological, surgical, clinical, and outcome data was assessed retrospectively. Surgical management was sorted according to three groups: decompression ( ), decompression and posterior instrumentation ( ), and decompression and 360° instrumentation with vertebral body replacement ( ). Sole biopsies or kypho-/vertebroplasties were excluded.
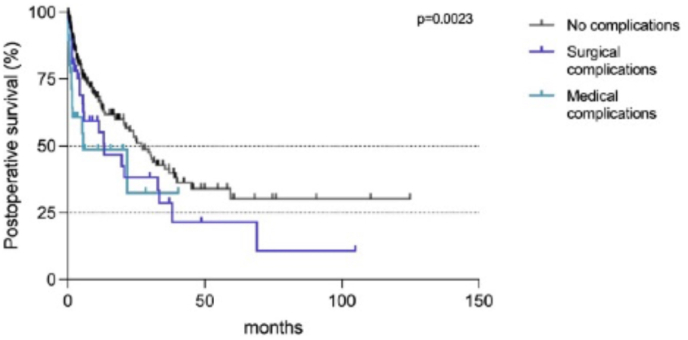
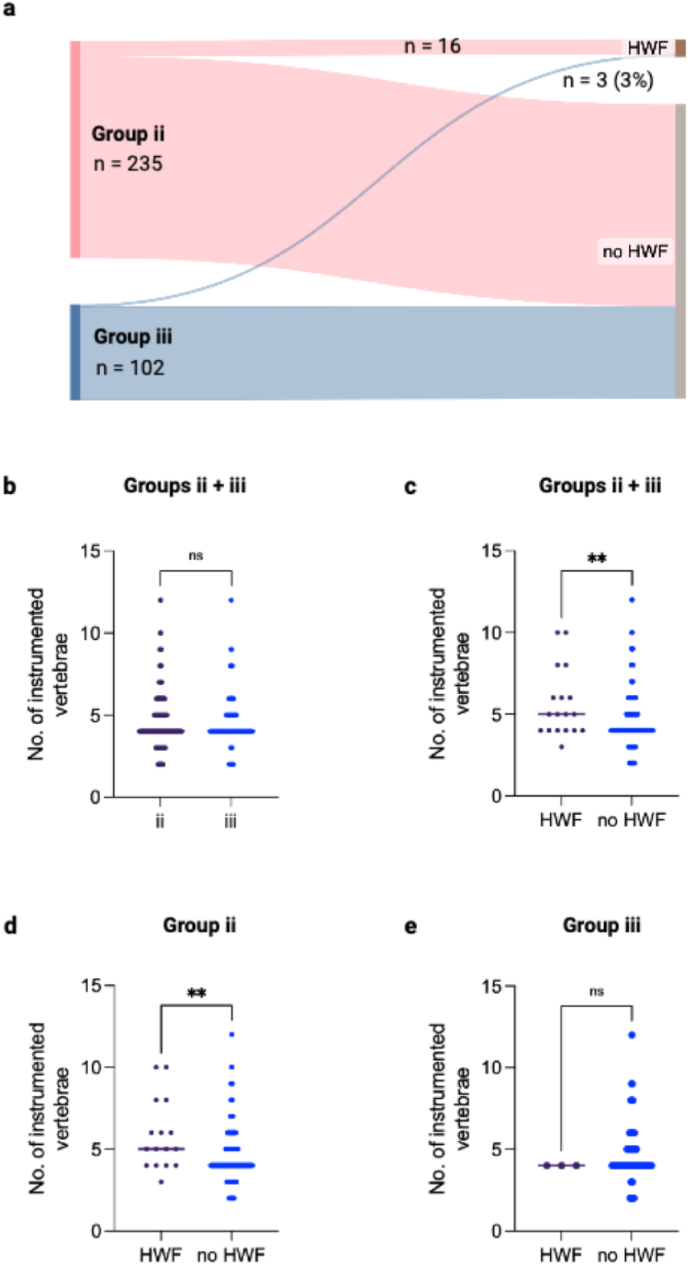
The inclusion criteria was met by 396 patients, of which 59 (15%) were treated with decompression ( ), 235 (59%) with posterior instrumentation ( ), and 102 (26%) with additional vertebral body replacement ( ). The main factor for selection towards instrumentation was a higher SINS score (SINS 9 in , 10 in vs. 7 in , p < 0.0001). Surgical complications occurred in 55 cases (14%), slightly more frequent following instrumentations (15% vs. 8% , p = 0.427). Reoperations were necessary in 65 cases (16%), mostly due to SSI (n = 19, 29%), local recurrence (n = 15, 23%), and hardware failure (HWF) during follow-up (n = 9, 18%, , p = 0.7853). HWF occurred significantly more frequent in cases with multisegmental metastases at the TLJ (p = 0.0002) which were treated with longer constructs (p = 0.0092). Median postoperative survival was 10 months. The occurrence of complications reduced postoperative survival drastically in all groups (p = 0.0023).
In this large multicentric patient cohort with TLJ metastases, the majority of patients (85%) were treated with instrumented spine surgery. The main factor for patient selection towards instrumented surgery was a higher SINS score. Long instrumentations for multisegmental disease at the TLJ were identified with higher risk for hardware-failure during follow-up. In those patients, frequent follow-up imaging is warranted. As postoperative survival is drastically reduced by the occurrence of postoperative complications, it is imperative to carefully select the individually appropriate extent of surgery in order to avoid postoperative complications.
胸腰段交界处(TLJ)的脊柱转移瘤对脊柱稳定性构成重大风险,在手术治疗方面需要特殊考虑。由于肿瘤治疗方法的改进,患者生存期延长,这可能使广泛的内固定手术成为合理选择。
本研究的目的是分析一个大型多中心队列中TLJ转移瘤患者在手术决策、治疗及相关并发症方面的治疗标准。
2010年至2022年间在五个学术性三级脊柱中心纳入了接受手术治疗的TLJ脊柱转移瘤患者。对流行病学、手术、临床和结局数据进行回顾性评估。手术治疗分为三组:减压( )、减压及后路内固定( )、减压及椎体置换的360°内固定( )。单纯活检或椎体后凸成形术/椎体成形术被排除。
396例患者符合纳入标准,其中59例(15%)接受减压治疗( ),235例(59%)接受后路内固定治疗( ),102例(26%)接受额外椎体置换治疗( )。选择内固定的主要因素是较高的SINS评分( 组为9分, 组为10分,而 组为7分,p<0.0001)。55例(14%)发生手术并发症,内固定术后略更常见( 组为15%, 组为8%,p = 0.427)。65例(16%)需要再次手术,主要原因是术后手术部位感染(n = 19,29%)、局部复发(n = 15,23%)和随访期间内固定失败(HWF,n = 9,18%, ,p = 0.7853)。TLJ多节段转移瘤患者中HWF发生率显著更高(p = 0.0002),且使用更长内固定装置治疗的患者中HWF发生率更高(p = 0.0092)。术后中位生存期为10个月。所有组中并发症的发生均显著降低了术后生存期(p = 0.0023)。
在这个大型多中心TLJ转移瘤患者队列中,大多数患者(85%)接受了脊柱内固定手术。选择内固定手术的主要因素是较高的SINS评分。TLJ多节段疾病的长节段内固定在随访期间内固定失败风险更高。对于这些患者,需要频繁进行随访影像学检查。由于术后并发症的发生会显著降低术后生存期,因此必须谨慎选择个体合适的手术范围以避免术后并发症。