Sławek-Szmyt Sylwia, Stępniewski Jakub, Kurzyna Marcin, Klaudel Jacek, Kuliczkowski Wiktor, Lewandowski Maciej, Grabka Marek, Roik Marek, Ordiene Rasa, Jankiewicz Stanisław, Kopeć Grzegorz, Darocha Szymon, Mroczek Ewa, Widecka Katarzyna, Kurzyna Paweł, Lesiak Maciej, Pruszczyk Piotr, Araszkiewicz Aleksander
1st Department of Cardiology, Poznan University of Medical Sciences, Poznan, Poland.
Department of Cardiac and Vascular Diseases, Jagiellonian University Medical College, John Paul II Hospital, Krakow, Poland.
Respir Res. 2025 Mar 5;26(1):87. doi: 10.1186/s12931-025-03162-4.
Data on interventional treatment of intermediate-high (and high-risk pulmonary embolism (PE) are limited. The authors sought to evaluate the safety and efficacy of catheter-directed mechanical aspiration thrombectomy (CDMT) in a real-world PE patient population.
This multicenter, prospective registry enrolled PE patients treated with CDMT using the Lightning 12 System. The primary safety endpoints included in-hospital all-cause mortality, procedure-related major bleeding, clinical deterioration, or bailout to another strategy. The primary efficacy outcomes included the reduction of pulmonary arterial pressures and change in the right-to-left ventricular (RV/LV) ratio 48 h after the CDMT. Multivariate regression analyzed characteristics associated with RV/LV improvement.
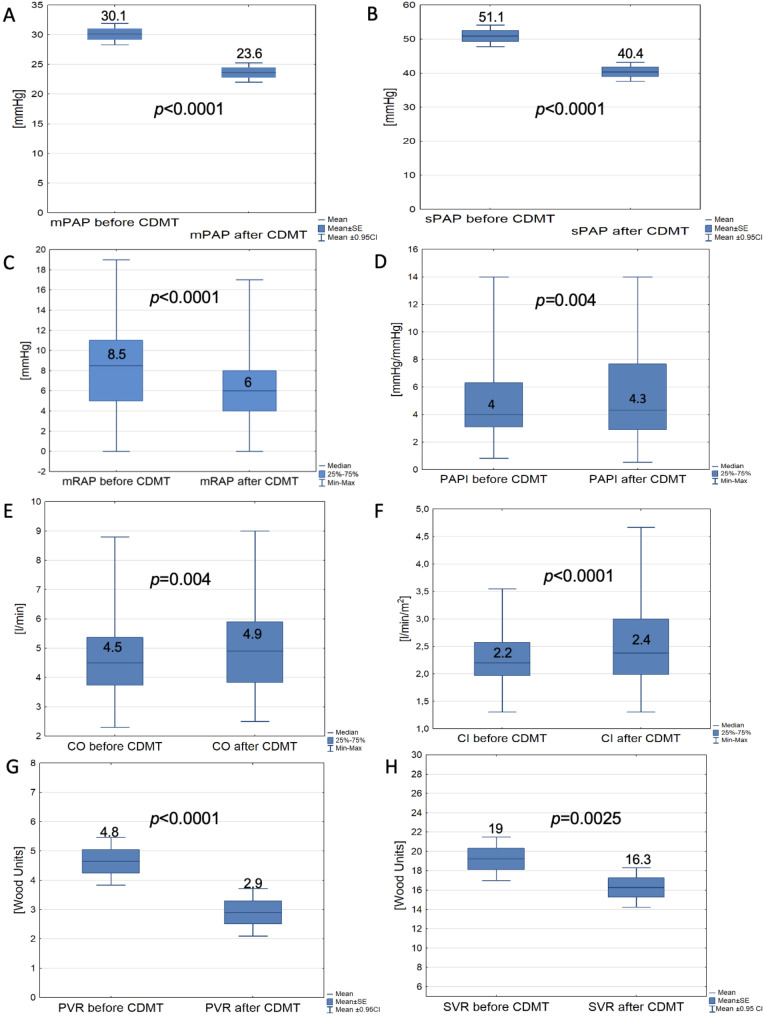
Our analysis included 150 patients, 72% with intermediate-high PE and 28% with high-risk PE. Systemic thrombolysis was contraindicated in 33.3%, whereas in 4% it failed. There were 2% intraprocedural deaths (1.3% due to RV failure and 0.7% due to massive interstitial bleeding), with no more deaths during follow-up. In 0.7%, CDMT was converted to open surgery, and in 0.7%, bailout systemic thrombolysis and extracorporeal oxygenation support. Major bleedings occurred in 1.3% within 48 h post CDMT. Immediate hemodynamic improvements included a mean 11.3±10 mmHg (22.1%) drop in systolic pulmonary arterial pressure (p < 0.0001) and a median 0.33 (0.25-0.45), (25.2%) drop in RV/LV ratio (p < 0.0001 for paired values), CONCLUSIONS: Aspiration thrombectomy with the Lightning 12 system characterizes an acceptable safety profile, substantial improvements in hemodynamic outcomes, and low mortality for patients with intermediate-high and high-risk PE.
NCT04879069 - date of registration 04.05.2021.
关于中高危(及高危)肺栓塞(PE)介入治疗的数据有限。作者旨在评估在真实世界的PE患者群体中导管定向机械吸栓术(CDMT)的安全性和有效性。
这项多中心前瞻性注册研究纳入了使用Lightning 12系统接受CDMT治疗的PE患者。主要安全终点包括院内全因死亡率、与手术相关的大出血、临床恶化或改用另一种治疗策略。主要疗效指标包括CDMT术后48小时肺动脉压的降低以及右心室与左心室(RV/LV)比值的变化。多变量回归分析了与RV/LV改善相关的特征。
我们的分析纳入了150例患者,其中72%为中高危PE,28%为高危PE。33.3%的患者存在全身溶栓禁忌证,4%的患者溶栓失败。术中死亡2%(1.3%死于右心室衰竭,0.7%死于大量间质出血),随访期间无更多死亡病例。0.7%的患者CDMT转为开放手术,0.7%的患者改用全身溶栓和体外氧合支持。CDMT术后48小时内大出血发生率为1.3%。即刻血流动力学改善包括收缩期肺动脉压平均下降11.3±10 mmHg(22.1%)(p < 0.0001),RV/LV比值中位数下降0.33(0.25 - 0.45)(25.2%)(配对值p < 0.0001)。结论:使用Lightning 12系统进行吸栓术具有可接受的安全性、血流动力学结果显著改善以及中高危和高危PE患者死亡率低的特点。
NCT04879069 - 注册日期2021年5月4日。