Bar Yael, Fell Geoffrey, Dedeoglu Aylin, Moffett Natalie, Vidula Neelima, Spring Laura, Wander Seth A, Bardia Aditya, Ko Naomi, Moy Beverly, Ellisen Leif W, Isakoff Steven J
Massachusetts General Hospital Cancer Center, Boston, MA, USA.
Tel Aviv Sourasky Medical Center and The Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel.
NPJ Breast Cancer. 2025 Mar 11;11(1):27. doi: 10.1038/s41523-025-00741-y.
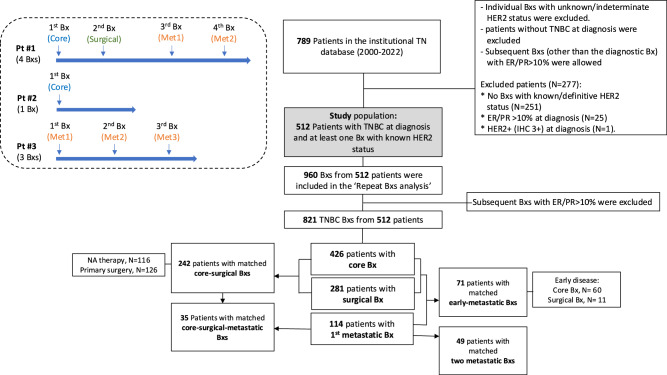
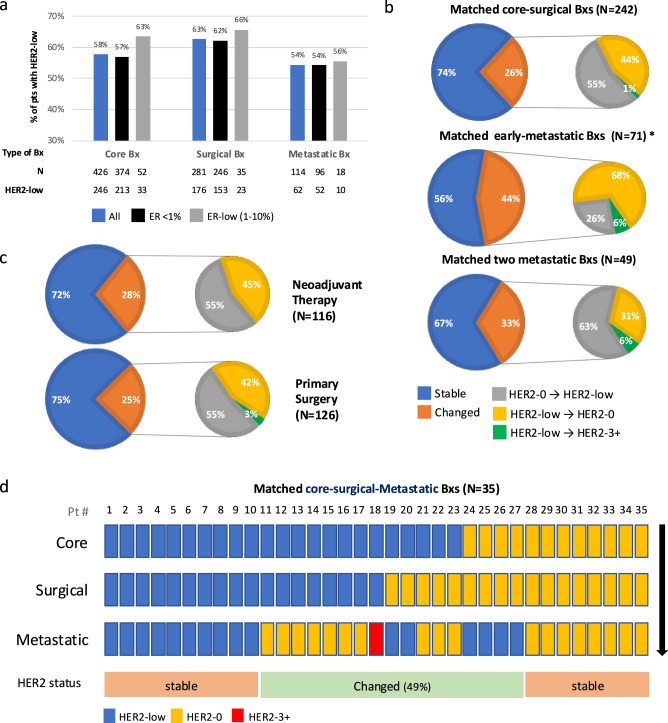
Trastuzumab deruxtecan (T-DXd) is approved for HER2-low (HER2 immunohistochemistry (IHC)1+ or 2+ with non-amplified in situ hybridization (ISH)), but not HER2-0 (IHC 0) metastatic breast cancer. The impact of repeat biopsies (Bxs) in identifying new potential candidates with triple negative breast cancer (TNBC) for T-DXd treatment remains unknown. 512 consecutive patients with TNBC at diagnosis were included in the study cohort. Bxs were categorized as core, surgical, or metastatic based on the timing and method of biopsy (Bx) acquisition, and the total number of Bxs was determined for each patient. Additionally, matched biopsies were identified, and the rate of discordance in HER2 status was calculated. The proportion of patients with at least one HER2-low result increased as the number of successive Bxs increased [59%, 73%, 83%, 83%, and 100% when 1 (196 patients), 2 (231 patients), 3 (48 patients), 4 (29 patients), and ≥ 5 (8 patients) Bxs were obtained, respectively]. Among patients without a prior HER2-low result, approximately one-third demonstrated HER2-low status with each additional successive Bx. HER2 status exhibited variability between matched Bxs, with observed discordance rates of 26%, 44%, and 33% between matched core-surgical, early-metastatic, and two metastatic matched Bxs, respectively. Our findings indicate that HER2 status can vary between different Bxs taken during the disease course of patients with TNBC with the highest discordance rate observed between the primary and metastatic Bxs. For patients with metastastic HER2-0 TNBC, repeat Bxs can increase the chance of obtaining a HER2-low result, thereby offering patients a promising therapeutic option.
德曲妥珠单抗(T-DXd)被批准用于治疗HER2低表达(HER2免疫组化(IHC)1+或2+且原位杂交(ISH)未扩增)的转移性乳腺癌,但不适用于HER2阴性(IHC 0)的转移性乳腺癌。重复活检在识别新的三阴性乳腺癌(TNBC)潜在候选者以接受T-DXd治疗方面的影响尚不清楚。512例连续诊断为TNBC的患者被纳入研究队列。根据活检获取的时间和方法,将活检分为粗针活检、手术活检或转移灶活检,并确定每位患者的活检总数。此外,识别匹配的活检样本,并计算HER2状态的不一致率。随着连续活检次数的增加,至少有一次HER2低表达结果的患者比例增加[当分别进行1次(196例患者)、2次(231例患者)、3次(48例患者)、4次(29例患者)和≥5次(8例患者)活检时,比例分别为59%、73%、83%、83%和100%]。在之前没有HER2低表达结果的患者中,每增加一次连续活检,约三分之一的患者表现出HER2低表达状态。HER2状态在匹配的活检样本之间存在变异性,在匹配的粗针活检与手术活检、早期转移灶活检以及两个转移灶匹配活检之间,观察到的不一致率分别为26%、44%和33%。我们的研究结果表明,在TNBC患者的疾病过程中,不同活检样本之间的HER2状态可能会有所不同,其中原发灶和转移灶活检之间的不一致率最高。对于转移性HER2阴性TNBC患者,重复活检可增加获得HER2低表达结果的机会,从而为患者提供有前景的治疗选择。