Aldli Mohammad, Alsultan Mohammad, Alkhatib MhdAmin
Department of cardiology, Damascus University- Faculty of Medicine, Damascus, Syria.
Department of Nephrology, Damascus University- Faculty of Medicine, Omar Ibn Abdulaziz Street, Al Mazah, Damascus, Syria.
BMC Cardiovasc Disord. 2025 Mar 18;25(1):194. doi: 10.1186/s12872-025-04644-5.
To compare the clinical characteristics and outcomes of patients with acute heart failure (AHF) according to the 2016 European Society of Cardiology (ESC) guidelines taking into account isolated right HF (RHF) with left HF (LHF) phenotypes. Volume status was assessed by the clinical manifestations and lung ultrasound (LUS). The secondary aim was to study the role of echocardiography in congestion based on LUS and their relations with outcomes.
This study included AHF patients, who referred to the emergency department (ED) at AL-Mouwasat and AL-Assad University Hospitals in Syria between May and August 2024. The same cardiologist reviewed medical reports, signs/ symptoms of decompensation, echocardiographic assessment, diagnosis, and treatment therapies.
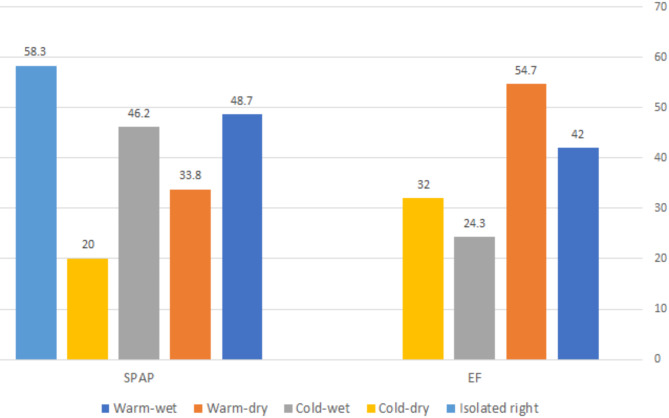
Of 100 patients, 10 patients (10%) had isolated RHF and 90 patients (90%) had LHF, including warm-wet (n = 65, 65%), followed by cold-wet (n = 13, 13%), warm-dry (n = 10, 10%), and cold-dry (n = 2, 2%). Most discharged patients without admission were Warm-dry, meanwhile most of patients with cold-wet (76.9%) were admitted to intensive care unit (ICU). The longest in-hospital stays were in cold-wet (11.9 days) followed by isolated RHF (7.5 days). While in-hospital mortality was mainly in cold-wet (38.5%) followed by isolated RHF (20%). Diuretics dose was highest in cold-wet followed by isolated RHF, while hydration was predominantly in cold-wet. Using vasopressors and inotropes were predominantly in cold-wet. Systolic blood pressure (SBP), hemoglobin (Hb), sodium (Na), proximal right ventricular outflow tract (RVOT1), left ventricular end-diastolic internal diameter (LVIDd), Tricuspid annular systolic plane excursion (TAPSE), and systolic pulmonary atrial pressure (SPAP) correlated with hospital stays, while only SBP and Cr correlated with in-hospital mortality. The cut-off values of E/e' ratio, isovolumic relaxation time (IVRT), and deceleration time (DT) were (12.5, 55ms, and 131.5 ms; respectively) and could predict congestion (guided by LUS) with sensitivities of (96%, 74%, and 62%; respectively) and specificities of (53%, 92%, and 84%; respectively).
Classifying AHF patients into these five groups, based on clinical examination supporting by echocardiography and LUS evaluation can give better assessment of the AHF phenotypes and gives more details for management. The bedside diagnostic assessment by LUS and echocardiography is an easy tool and seems to be of great benefit in detecting congestion that enhances the treatment protocols.
根据2016年欧洲心脏病学会(ESC)指南,比较急性心力衰竭(AHF)患者的临床特征和预后,同时考虑孤立性右心衰竭(RHF)与左心衰竭(LHF)表型。通过临床表现和肺部超声(LUS)评估容量状态。次要目的是研究基于LUS的超声心动图在充血中的作用及其与预后的关系。
本研究纳入了2024年5月至8月期间转诊至叙利亚穆瓦萨特和阿萨德大学医院急诊科的AHF患者。由同一位心脏病专家审查医疗报告、失代偿的体征/症状、超声心动图评估、诊断和治疗方法。
100例患者中,10例(10%)为孤立性RHF,90例(90%)为LHF,包括暖湿型(n = 65,65%),其次是冷湿型(n = 13,13%)、暖干型(n = 10,10%)和冷干型(n = 2,2%)。大多数未住院的出院患者为暖干型,而大多数冷湿型患者(76.9%)入住重症监护病房(ICU)。住院时间最长的是冷湿型(11.9天),其次是孤立性RHF(7.5天)。院内死亡率主要发生在冷湿型(38.5%),其次是孤立性RHF(20%)。利尿剂剂量在冷湿型中最高,其次是孤立性RHF,而补液主要在冷湿型。使用血管升压药和正性肌力药主要在冷湿型。收缩压(SBP)、血红蛋白(Hb)、钠(Na)、右心室流出道近端(RVOT1)、左心室舒张末期内径(LVIDd)、三尖瓣环收缩期平面位移(TAPSE)和收缩期肺动脉压(SPAP)与住院时间相关,而只有SBP和肌酐与院内死亡率相关。E/e'比值、等容舒张时间(IVRT)和减速时间(DT)的截断值分别为(12.5、55ms和131.5ms),可以预测充血(以LUS为指导),敏感性分别为(96%、74%和62%),特异性分别为(53%、92%和84%)。
基于超声心动图和LUS评估支持的临床检查,将AHF患者分为这五组,可以更好地评估AHF表型,并为管理提供更多细节。LUS和超声心动图的床旁诊断评估是一种简单的工具,似乎在检测充血方面有很大益处,可优化治疗方案。