Hsu Henry R, Sekhar Praba, Grover Jahnavi, Tian David H, Downey Ciaran, Maudlin Ben, Dissanayake Chathuri, Dennis Mark
School of Medicine, University of Sydney, Sydney, New South Wales, Australia.
Department of Anaesthesia and Perioperative Medicine, Westmead Hospital, Sydney, New South Wales, Australia.
PLoS One. 2025 Mar 19;20(3):e0310289. doi: 10.1371/journal.pone.0310289. eCollection 2025.
Venoarterial extracorporeal membrane oxygenation (V-A ECMO) use to support patients in cardiac failure is increasing. Despite this increased use, predicting successful weaning from ECMO can be challenging, no uniform guidelines on weaning exist. Therefore, we completed a systematic review to evaluate prognostic factors that predict successful weaning from V-A ECMO.
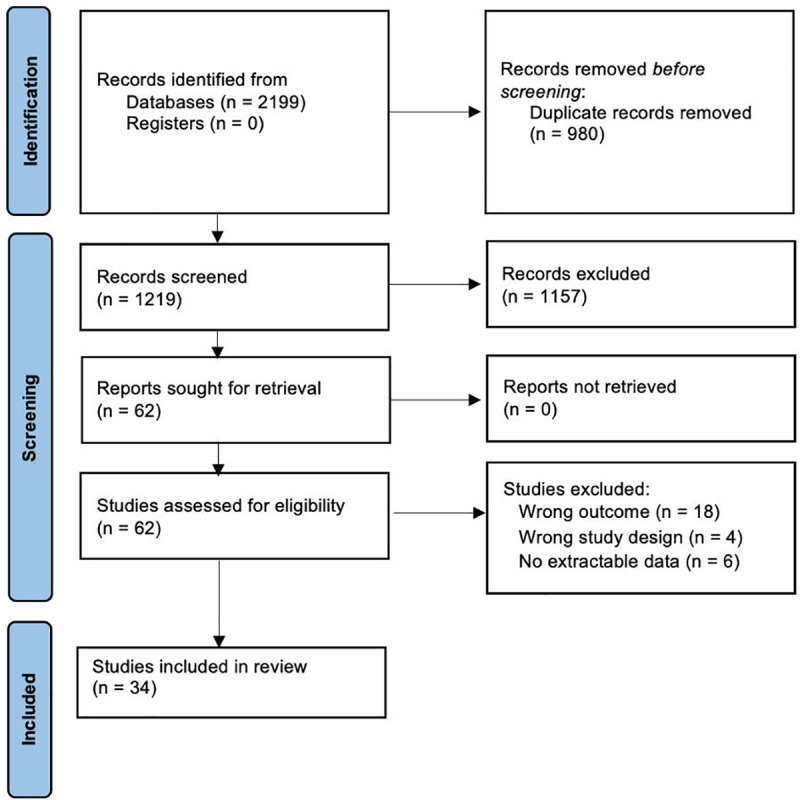
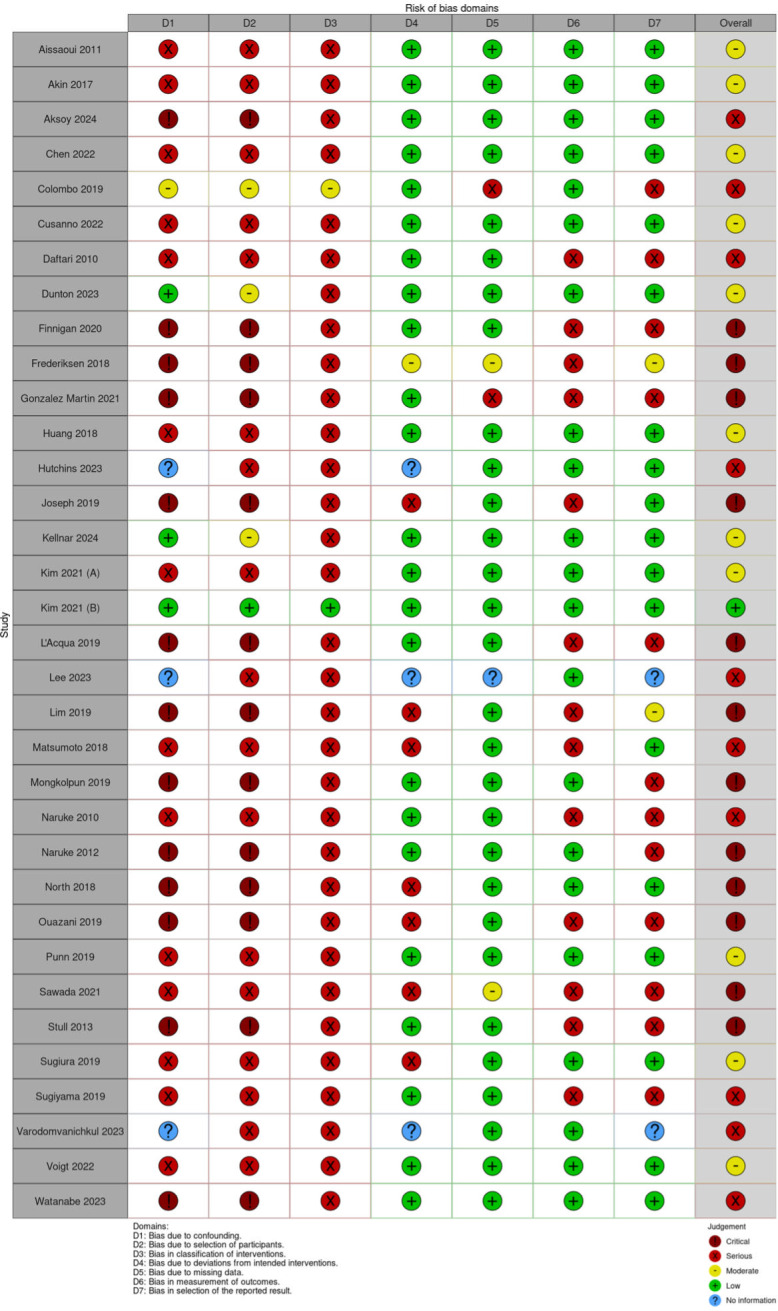
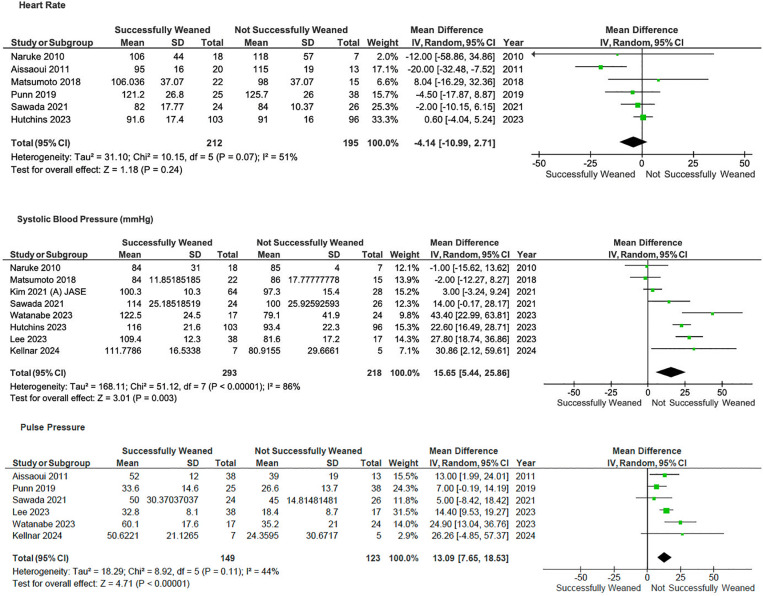
Following the PRIMSA guidelines, a systematic literature search of Medline, Embase, SCOPUS and CENTRAL identified original research studies of patients requiring V-A ECMO where weaning was attempted. Data was collected on demographic factors and weaning protocol, biomarkers, haemodynamic, echocardiographic factors for the successfully weaned (SW) and not successfully weaned (NSW) groups. Two investigators reviewed studies for relevance, extracted data, and assessed risk of bias using the ROBINS-I tool. The study was registered on the international prospective register of systematic reviews (PROSPERO ID# CRD42022366153).
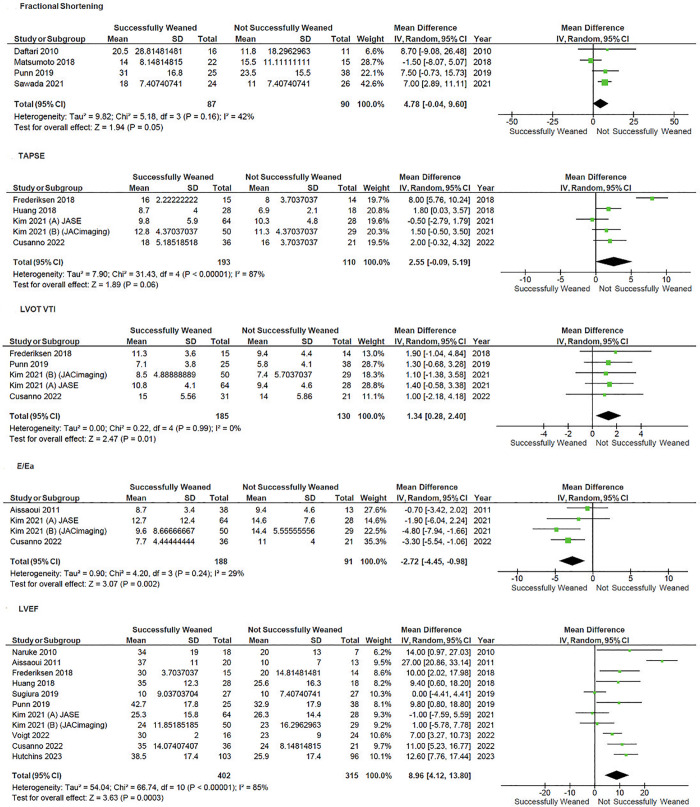
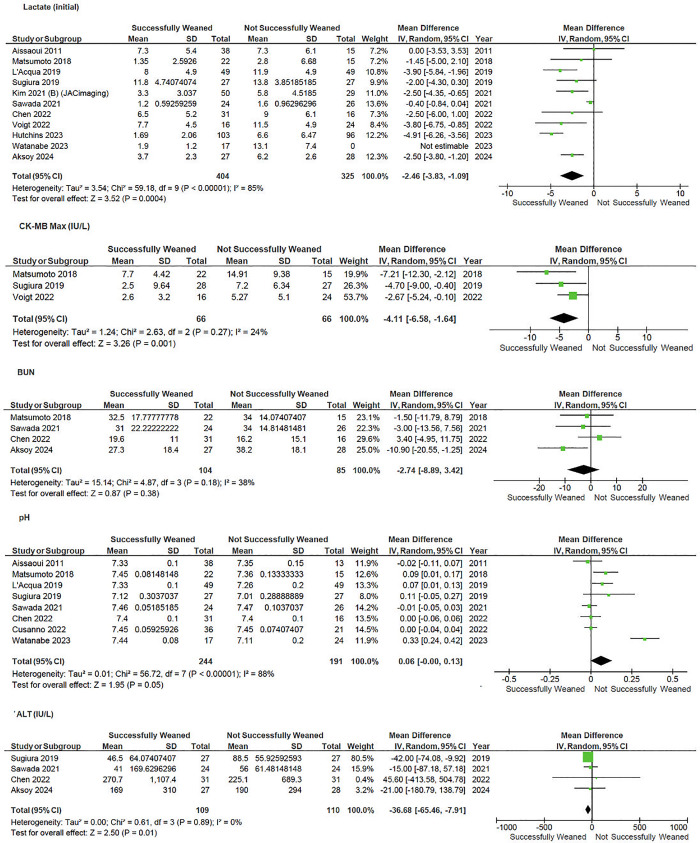
1219 records were screened, of which 20 studies were deemed sufficient to be included in the statistical analysis based on pre-specified criteria. Factors associated with successful weaning were higher left ventricular ejection fraction (LVEF) (MD 9.0, 95% CI 4.1-13.8; p < 0.001) and left ventricular outflow tract velocity time integral (LVOT VTI) at time of weaning, (MD 1.35, 95% CI 0.28-2.40 lactate at admission (MD -3.2, 95% CI -4.8 to -1.5, p < 0.001), and CK-MB at admission (MD -4.11, 95%CI -6.6 to -1.6, p = 0.001). Critical appraisal demonstrated moderate-high risk of bias owing to confounding and low sample sizes.
In patients on V-A ECMO support being assessed for weaning multi-parametric assessment is required. Moderate-high heterogeneity and low sample sizes warrant higher-quality studies to help guide decisions to wean patients from V-A ECMO.
用于支持心力衰竭患者的静脉-动脉体外膜肺氧合(V-A ECMO)的使用正在增加。尽管使用量增加,但预测能否成功脱离ECMO可能具有挑战性,目前尚无关于撤机的统一指南。因此,我们完成了一项系统评价,以评估预测V-A ECMO成功撤机的预后因素。
按照PRISMA指南,对Medline、Embase、SCOPUS和CENTRAL进行系统文献检索,确定了尝试撤机的需要V-A ECMO的患者的原始研究。收集了成功撤机(SW)组和未成功撤机(NSW)组的人口统计学因素、撤机方案、生物标志物、血流动力学、超声心动图因素的数据。两名研究人员审查研究的相关性,提取数据,并使用ROBINS-I工具评估偏倚风险。该研究已在国际前瞻性系统评价注册库(PROSPERO ID# CRD42022366153)上注册。
共筛选了1219条记录,其中20项研究根据预先设定的标准被认为足以纳入统计分析。与成功撤机相关的因素包括较高的左心室射血分数(LVEF)(MD 9.0,95%CI 4.1-13.8;p<0.001)和撤机时的左心室流出道速度时间积分(LVOT VTI)(MD 1.35,95%CI 0.28-2.40)、入院时的乳酸水平(MD -3.2,95%CI -4.8至-1.5,p<0.001)以及入院时的肌酸激酶同工酶(CK-MB)(MD -4.11,95%CI -6.6至-1.6,p = 0.001)。批判性评价表明,由于存在混杂因素和样本量较小,存在中度至高度偏倚风险。
对于接受V-A ECMO支持并正在评估撤机的患者,需要进行多参数评估。中度至高度的异质性和较小的样本量需要更高质量的研究来帮助指导V-A ECMO患者撤机的决策。