Department of Anesthesia, Intensive Care and Perioperative Care Medicine, Rangueil University Hospital, Toulouse, France.
Medical Intensive Care Unit, Hôpital Cochin, AP-HP, Paris, France.
Sci Rep. 2022 Aug 16;12(1):13842. doi: 10.1038/s41598-022-18105-y.
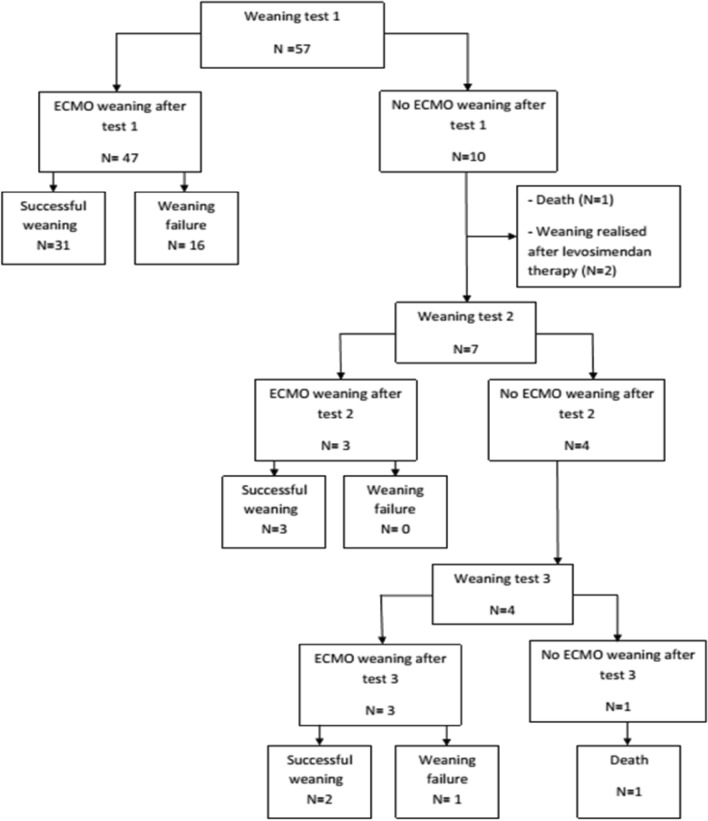
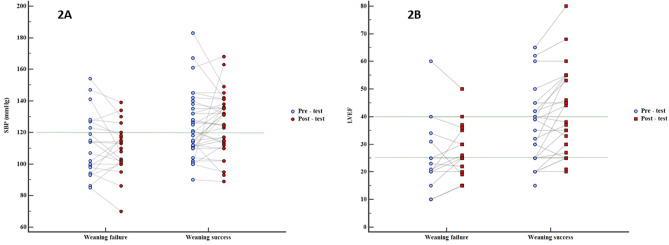
The use of veno-arterial extracorporeal membrane oxygenation (VA ECMO) for the treatment of refractory cardiogenic shock has increased significantly. Nevertheless, early weaning may be advisable to reduce the potential for severe complications. Only a few studies focusing on ECMO weaning predictors are currently available. Our objective was to evaluate factors that may help predict failure during VA ECMO weaning. We included 57 patients on VA ECMO support previously considered suitable for weaning based on specific criteria. Clinical, haemato-chemical and echocardiographic assessment was considered before and after a "weaning test" (ECMO flow < 2 L/min for at least 60 min). ECMO removal was left to the discretion of the medical team blinded to the results. Weaning failure was defined as a patient who died or required a new VA ECMO, heart transplant or LVAD 30 days after ECMO removal. Thirty-six patients (63.2%) were successfully weaned off VA ECMO, of whom 31 (54.4%) after the first weaning test. In case of first test failure, 3 out of 7 patients could be weaned after a 2nd test and 3 out of 4 patients after a 3rd test. Pre-existing ischemic heart disease (OR 9.6 [1.1-83]), pre-test left ventricular ejection fraction (LVEF) ≤ 25% and/or post-test LVEF ≤ 40% (OR 11 [0.98-115]), post-test systolic blood pressure ≤ 120 mmHg (OR 33 [3-385]), or length of ECMO support > 7 days (OR 24 [2-269]) were predictors of weaning failure. The VA ECMO weaning test failed in less than 40% of patients considered suitable for weaning. Clinical and echocardiographic criteria, which are easily accessible by a non-expert intensivist, may help increase the probability of successful weaning.
体外膜肺氧合(VA ECMO)在治疗难治性心源性休克中的应用显著增加。然而,早期脱机会降低严重并发症的风险。目前只有少数研究关注 ECMO 脱机预测因素。我们的目的是评估可能有助于预测 VA ECMO 脱机失败的因素。我们纳入了 57 名先前根据特定标准被认为适合脱机的 VA ECMO 支持患者。在进行“脱机测试”(ECMO 流量<2 L/min 至少 60 min)前后,进行临床、血液化学和超声心动图评估。ECMO 去除由对结果不知情的医疗团队决定。将脱机失败定义为 ECMO 去除后 30 天内死亡或需要新的 VA ECMO、心脏移植或 LVAD 的患者。36 名患者(63.2%)成功脱机,其中 31 名(54.4%)在第一次脱机测试后。如果第一次测试失败,7 名患者中有 3 名可以在第二次测试后脱机,4 名患者中有 3 名可以在第三次测试后脱机。存在缺血性心脏病(OR 9.6 [1.1-83])、测试前左心室射血分数(LVEF)≤25%和/或测试后 LVEF≤40%(OR 11 [0.98-115])、测试后收缩压≤120 mmHg(OR 33 [3-385])或 ECMO 支持时间>7 天(OR 24 [2-269])是脱机失败的预测因素。考虑到适合脱机的患者中,不到 40%的患者在 VA ECMO 脱机测试中失败。临床和超声心动图标准,这些标准易于非专家重症监护医生获得,可能有助于提高成功脱机的概率。