Antehunegn Tesema Getayeneh, Sarfo Michael, Okeke Sylvester R, Ameyaw Edward Kwabena, Yaya Sanni
Department of Epidemiology and Biostatistics, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia.
School of Human and Health Sciences, University of Huddersfield, United Kingdom.
PLoS One. 2025 Mar 19;20(3):e0316884. doi: 10.1371/journal.pone.0316884. eCollection 2025.
Childhood vaccination is a highly cost-effective strategy for preventing vaccine-preventable diseases, including poliomyelitis. Despite advancements in vaccination coverage across Africa, polio remains a public health concern. Limited multi-country analyses on oral polio vaccine (OPV) dropout in African nations hinder the development of context-specific interventions. This study investigates OPV uptake and associated factors in sub-Saharan Africa (SSA).
This study analyzed data from the Demographic and Health Surveys of 37 sub-Saharan African countries, encompassing 60,846 children aged 12-23 months. Multilevel multinomial logistic regression models were employed to explore associations between individual- and community-level factors and vaccination status, categorized as non-vaccinated, dropout, or fully vaccinated. Four nested models were assessed, with the model exhibiting the lowest deviance (-2 Log-likelihood Ratio (-2LLR)) identified as the best fit. Variables with p-values < 0.2 in bivariable analysis were included in the multivariable analysis. The adjusted Relative Risk Ratios (aRRR) with 95% Confidence Intervals (CI) were reported to determine statistical significance and the strength of associations.
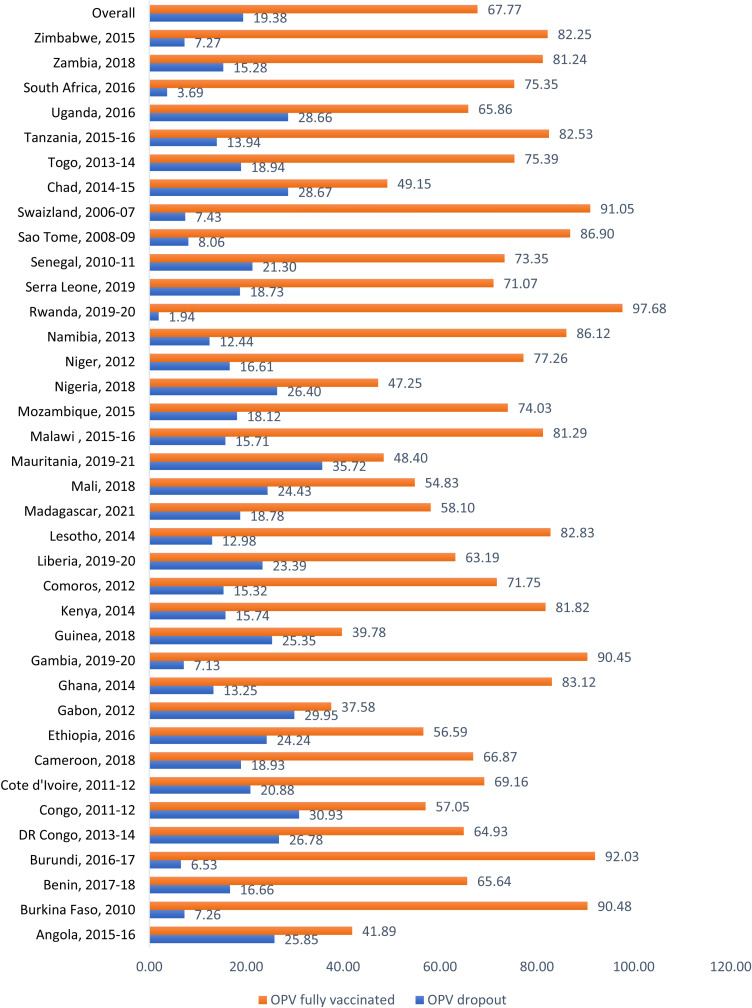
Among children aged 12-23 months, OPV1, OPV2, and OPV3 coverage rates were 86.59%, 81.27%, and 68.41%, respectively. The prevalence of OPV dropout and full vaccination in SSA were 19.38% (95% CI: 19.06%, 19.69%) and 67.77% (95% CI: 67.40%, 68.14%), respectively, with a dropout rate of 20.98%. Key factors significantly associated with non-vaccination included maternal education (primary: aRRR = 0.58; secondary: aRRR = 0.64; higher: aRRR = 0.75), household wealth (poorer: aRRR = 0.91; middle: aRRR = 0.82; richer: aRRR = 0.70), maternal age (20-29: aRRR = 0.67; 30-39: aRRR = 0.60; 40-49: aRRR = 0.59), health facility delivery (aRRR = 0.28), media exposure (aRRR = 0.64), marital status (currently married: aRRR = 0.87), parity (2-3 births: aRRR = 1.11), and rural residence (aRRR = 0.73). Regional disparities revealed higher risks of non-vaccination and dropout in Southern, Central, and West Africa compared to East Africa.
This study highlights the multifaceted determinants of oral polio vaccination dropout in SSA. Targeted interventions, such as improving maternal education, enhancing access to healthcare facilities, addressing socioeconomic inequalities, and mitigating regional disparities, are essential to boosting vaccination coverage and preventing polio resurgence. Focused efforts in Western and Central Africa are critical to sustaining and expanding vaccination programs.
儿童疫苗接种是预防包括脊髓灰质炎在内的可通过疫苗预防疾病的一项极具成本效益的策略。尽管非洲各地的疫苗接种覆盖率有所提高,但脊髓灰质炎仍然是一个公共卫生问题。对非洲国家口服脊髓灰质炎疫苗(OPV)接种中断情况的多国分析有限,这阻碍了针对具体情况的干预措施的制定。本研究调查了撒哈拉以南非洲(SSA)地区OPV的接种情况及相关因素。
本研究分析了37个撒哈拉以南非洲国家的人口与健康调查数据,涵盖60846名12至23个月大的儿童。采用多水平多项逻辑回归模型来探究个体和社区层面因素与疫苗接种状况之间的关联,疫苗接种状况分为未接种、接种中断和全程接种。评估了四个嵌套模型,将偏差最低(-2对数似然比(-2LLR))的模型确定为最佳拟合模型。在双变量分析中p值<0.2的变量纳入多变量分析。报告了调整后的相对风险比(aRRR)及其95%置信区间(CI),以确定统计显著性和关联强度。
在12至23个月大的儿童中,OPV1、OPV2和OPV3的接种率分别为86.59%、81.27%和68.41%。SSA地区OPV接种中断和全程接种的患病率分别为19.38%(95%CI:19.06%,19.69%)和67.77%(95%CI:67.40%,68.14%),接种中断率为20.98%。与未接种显著相关的关键因素包括母亲教育程度(小学:aRRR = 0.58;中学:aRRR = 0.64;高等:aRRR = 0.75)、家庭财富(较贫困:aRRR = 0.91;中等:aRRR = 0.82;较富裕:aRRR = 0.70)、母亲年龄(20 - 29岁:aRRR = 0.67;30 - 39岁:aRRR = 0.60;40 - 49岁:aRRR = 0.59)、在医疗机构分娩(aRRR = 0.28)、媒体曝光(aRRR = 0.64)、婚姻状况(目前已婚:aRRR = 0.87)、生育次数(2 - 3次分娩:aRRR = 1.11)以及农村居住(aRRR = 0.73)。区域差异显示,与东非相比,南部、中部和西非未接种和接种中断的风险更高。
本研究突出了SSA地区口服脊髓灰质炎疫苗接种中断的多方面决定因素。有针对性的干预措施,如提高母亲教育程度、增加获得医疗保健设施的机会、解决社会经济不平等问题以及减轻区域差异,对于提高疫苗接种覆盖率和预防脊髓灰质炎死灰复燃至关重要。在西非和中非集中开展努力对于维持和扩大疫苗接种计划至关重要。