Meffen Anna, Rutherford Mark J, Sayers Rob D, Houghton John S M, Bradbury Naomi, Gray Laura J
Department of Population Health Sciences, University of Leicester, Leicester, UK.
National Institute for Health and Care Research Leicester Biomedical Research Centre, University of Leicester, Leicester, UK.
BJS Open. 2025 Mar 4;9(2). doi: 10.1093/bjsopen/zraf004.
Peripheral artery disease and diabetes are the main primary risk factors for non-traumatic major lower limb amputation. Regional variation in incidence of major lower limb amputation has yet to be fully described in terms of these risk factors and explained. The aim of this study was to estimate yearly incidence of major lower limb amputation over a 10-year interval (2010-2019) across England, by related condition and by region and, additionally, to investigate reasons for regional variation.
This observational study utilized primary care (Clinical Practice Research Datalink Aurum), secondary care (Hospital Episode Statistics), death and demographic data in England. Adults registered with a practice using Clinical Practice Research Datalink Aurum and with Hospital Episode Statistics linkage were included. Patients with a record of major lower limb amputation during the interval 1 January 2010 to 31 December 2019 were identified and yearly incidence rates of major lower limb amputation were calculated. Co-morbidities analysed were cardiovascular disease (including coronary artery disease, peripheral artery disease and cerebrovascular disease), diabetes (of any type) and cancer. Demographic and socioeconomic covariates analysed were age, sex, ethnicity, deprivation level, region and urban/rural categorization.
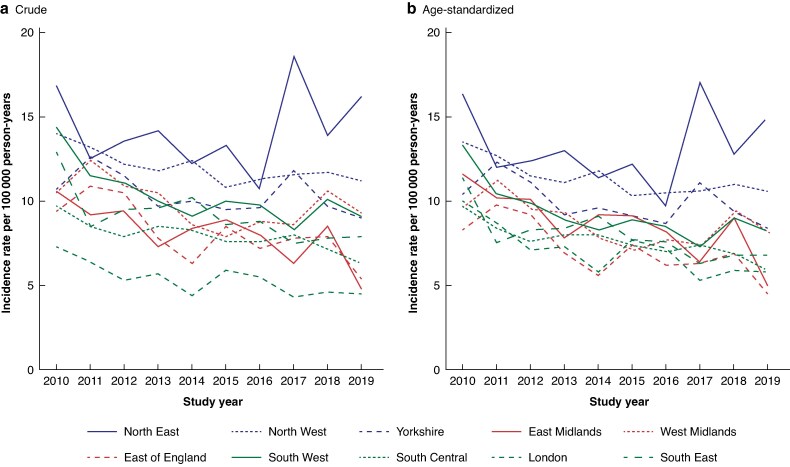
The study included 18 397 483 individuals, 8584 of which had a record of major lower limb amputation. The age-standardized yearly incidence rate of major lower limb amputation in England decreased by 30% from 11.2 per 100 000 person-years in 2010 to 7.8 in 2019. The incidence rate in those with diabetes fell by 30% over the 10-year interval, rose by 20% for those with both diabetes and cardiovascular disease, and changed little in those with cardiovascular disease. In 2019, the age-standardized incidence rate was highest in the North East (14.8 per 100 000 person-years) and lowest in the East of England (4.5 per 100 000 person-years). Between 2010 and 1019, incidence rates decreased across all regions, the largest decrease of 56% in the East Midlands and the smallest of 8% in the North East. Statistically significant regional variation remained after full adjustment for demographic, socioeconomic data and related conditions.
Whilst the incidence of major lower limb amputation is decreasing overall, significant regional variation in major lower limb amputation exists and is unexplained by demographic, socioeconomic and health data. Regional differences in service provision and accessibility should be investigated to provide further explanation.
外周动脉疾病和糖尿病是非创伤性主要下肢截肢的主要原发性危险因素。主要下肢截肢发病率的区域差异尚未根据这些危险因素得到充分描述和解释。本研究的目的是估计2010年至2019年这10年间英格兰主要下肢截肢的年发病率,按相关疾病和地区进行分类,此外,还调查区域差异的原因。
这项观察性研究利用了英格兰的初级医疗(临床实践研究数据链奥鲁姆)、二级医疗(医院事件统计)、死亡和人口数据。纳入了在使用临床实践研究数据链奥鲁姆的医疗机构注册且与医院事件统计有链接的成年人。确定了2010年1月1日至2019年12月31日期间有主要下肢截肢记录的患者,并计算了主要下肢截肢的年发病率。分析的合并症包括心血管疾病(包括冠状动脉疾病、外周动脉疾病和脑血管疾病)、糖尿病(任何类型)和癌症。分析的人口统计学和社会经济协变量包括年龄、性别、种族、贫困水平地区和城乡分类。
该研究纳入了18397483人,其中8584人有主要下肢截肢记录。英格兰主要下肢截肢的年龄标准化年发病率从2010年的每10万人年11.2例下降了30%,至2019年的7.8例。糖尿病患者的发病率在10年期间下降了30%,糖尿病和心血管疾病患者的发病率上升了20%,心血管疾病患者的发病率变化不大。2019年,年龄标准化发病率在东北部最高(每10万人年14.8例),在英格兰东部最低(每10万人年4.5例)。2010年至2019年期间,所有地区的发病率均下降,东米德兰兹降幅最大,为56%,东北部降幅最小,为8%。在对人口统计学、社会经济数据和相关疾病进行全面调整后,仍存在统计学上显著的区域差异。
虽然主要下肢截肢的发病率总体上在下降,但主要下肢截肢存在显著的区域差异,且人口统计学、社会经济和健康数据无法解释这种差异。应调查服务提供和可及性方面的区域差异,以提供进一步解释。