Lindman Brian R, Pibarot Philippe, Schwartz Allan, Oldemeyer J Bradley, Su Yan Ru, Goel Kashish, Cohen David J, Fearon William F, Babaliaros Vasilis, Daniels David, Chhatriwalla Adnan, Suradi Hussam S, Shah Pinak, Szerlip Molly, Mack Michael J, Dahle Thom, O'Neill William W, Davidson Charles J, Makkar Raj, Sheth Tej, Depta Jeremiah, DeVries James T, Southard Jeffrey, Pop Andrei, Sorajja Paul, Hahn Rebecca T, Zhao Yanglu, Leon Martin B, Généreux Philippe
Structural Heart and Valve Center (B.R.L.), Vanderbilt University Medical Center, Nashville, TN.
Division of Cardiovascular Medicine (B.R.L., Y.R.S., K.G.), Vanderbilt University Medical Center, Nashville, TN.
Circulation. 2025 Jun 3;151(22):1550-1564. doi: 10.1161/CIRCULATIONAHA.125.074425. Epub 2025 Mar 31.
The EARLY TAVR trial (Evaluation of TAVR Compared to Surveillance for Patients With Asymptomatic Severe Aortic Stenosis) demonstrated that early transcatheter aortic valve replacement (TAVR) intervention was superior to clinical surveillance with delayed TAVR in patients with asymptomatic severe aortic stenosis. Cardiac biomarkers are associated with maladaptive remodeling, symptom onset, and worse outcomes after TAVR. Whether elevated biomarkers identify asymptomatic patients more likely to benefit from early intervention is unknown.
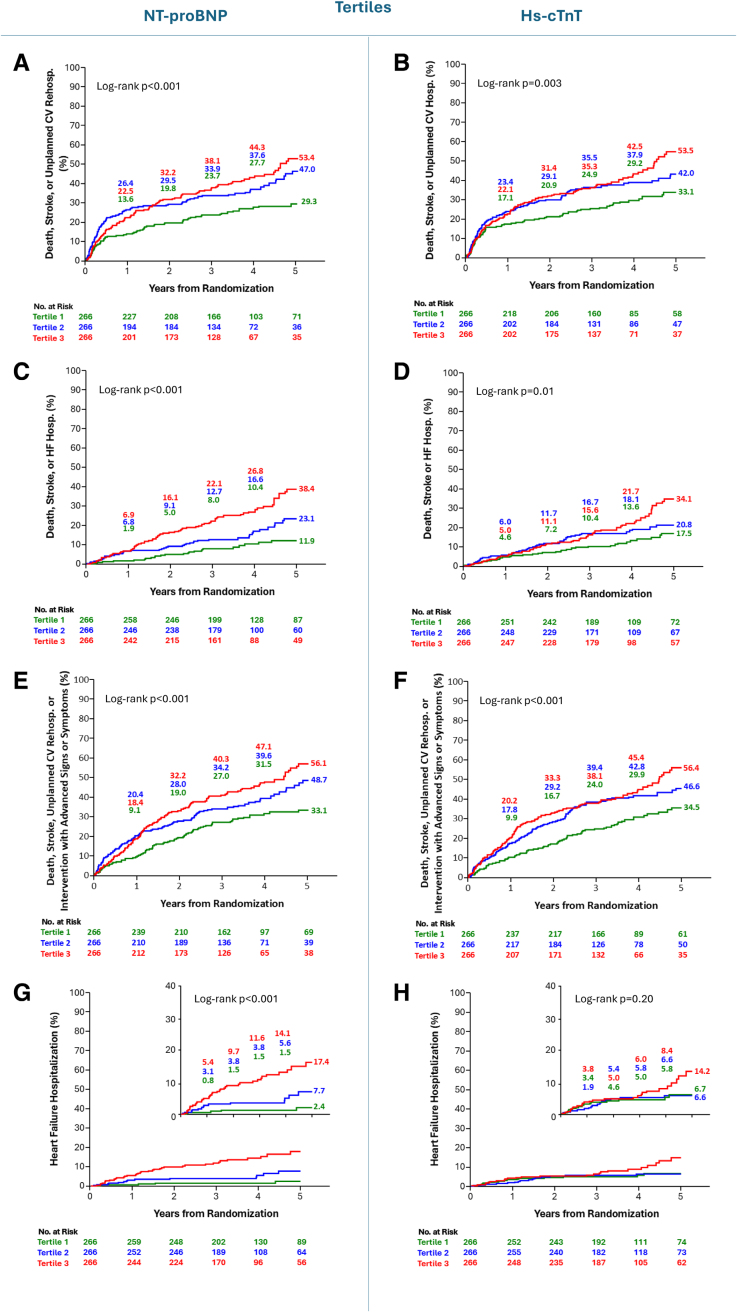
A core laboratory measured NT-proBNP (N-terminal pro-B-type natriuretic peptide) and high-sensitivity cardiac troponin T (hs-cTnT) levels. Associations between biomarker levels and risk of the trial primary end point (death, stroke, or unplanned cardiovascular hospitalization) and other secondary end points were examined with Kaplan-Meier curves and Cox proportional hazard models. Interaction tests were performed to assess whether the treatment effect of early TAVR, compared with clinical surveillance, differed according to biomarker levels.
Among 901 patients randomized in EARLY TAVR, 798 (89%) had biospecimens measured (median NT-proBNP level, 287 [145, 601]; median hs-cTnT level, 14.6 [10.5, 21.0]). Higher levels of NT-proBNP and hs-cTnT were broadly associated with higher event rates for multiple end points. In general, there was no significant interaction between baseline biomarkers and treatment group with respect to any composite or individual end point examined, although trends broadly demonstrated a greater relative benefit of early TAVR at lower biomarker levels. There was a significant interaction between hs-cTnT level and treatment group with respect to death or heart failure hospitalization ( =0.04) and heart failure hospitalization alone ( =0.03) such that the relative benefit of early TAVR was greater for patients with normal, rather than elevated, levels of hs-cTnT at baseline. For some end points, higher baseline NT-proBNP level was associated with numerically greater absolute risk reduction with early TAVR than were lower NT-proBNP levels.
In patients with asymptomatic severe high-gradient aortic stenosis, higher NT-proBNP and hs-cTnT levels were broadly associated with higher event rates, as expected. However, the relative benefit of an early TAVR strategy was consistent regardless of baseline biomarker levels and, contrary to our hypothesis, tended to be more pronounced in patients with the lowest biomarker levels. These findings suggest limited value for single measurements of these biomarkers to guide the timing of TAVR in asymptomatic patients.
URL: https://www.clinicaltrials.gov; Unique identifier: NCT03042104.
早期经导管主动脉瓣置换术(TAVR)试验(无症状严重主动脉瓣狭窄患者TAVR与观察的比较评估)表明,对于无症状严重主动脉瓣狭窄患者,早期经导管主动脉瓣置换术干预优于延迟TAVR的临床观察。心脏生物标志物与TAVR术后适应性不良重塑、症状发作及更差的预后相关。生物标志物升高是否能识别出更可能从早期干预中获益的无症状患者尚不清楚。
一个核心实验室检测了N末端B型利钠肽原(NT-proBNP)和高敏心肌肌钙蛋白T(hs-cTnT)水平。采用Kaplan-Meier曲线和Cox比例风险模型研究生物标志物水平与试验主要终点(死亡、卒中或非计划心血管住院)及其他次要终点风险之间的关联。进行交互检验以评估与临床观察相比,早期TAVR的治疗效果是否因生物标志物水平而异。
在早期TAVR试验随机分组的901例患者中,798例(89%)有生物标本检测结果(NT-proBNP水平中位数为287[145, 601];hs-cTnT水平中位数为14.6[10.5, 21.0])。NT-proBNP和hs-cTnT水平较高与多个终点的较高事件发生率广泛相关。总体而言,对于所检查的任何复合或单个终点,基线生物标志物与治疗组之间均无显著交互作用,尽管趋势大致表明在较低生物标志物水平时早期TAVR的相对获益更大。hs-cTnT水平与治疗组在死亡或心力衰竭住院(P = 0.04)及单独心力衰竭住院(P = 0.03)方面存在显著交互作用,因此对于基线hs-cTnT水平正常而非升高的患者,早期TAVR的相对获益更大。对于某些终点,较高的基线NT-proBNP水平与早期TAVR相比NT-proBNP水平较低时在数值上更大的绝对风险降低相关。
在无症状严重高梯度主动脉瓣狭窄患者中,NT-proBNP和hs-cTnT水平较高与较高事件发生率广泛相关,这与预期一致。然而,无论基线生物标志物水平如何,早期TAVR策略的相对获益是一致的,并且与我们的假设相反,在生物标志物水平最低的患者中往往更为明显。这些发现表明,单次测量这些生物标志物对于指导无症状患者TAVR的时机价值有限。