Tucci Alexandra, Cloutier Paula, Polihronis Christine, Kennedy Allison, Zemek Roger, Gray Clare, Reid Sarah, Pajer Kathleen, Gardner William, Barrowman Nicholas, Cappelli Mario, Jabbour Mona
Children's Hospital of Eastern Ontario (CHEO) Research Institute, Ottawa, ON, Canada.
Knowledge Institute on Child and Youth Mental Health and Addictions, Ottawa, ON, Canada.
BMC Health Serv Res. 2025 Mar 31;25(1):475. doi: 10.1186/s12913-025-12524-z.
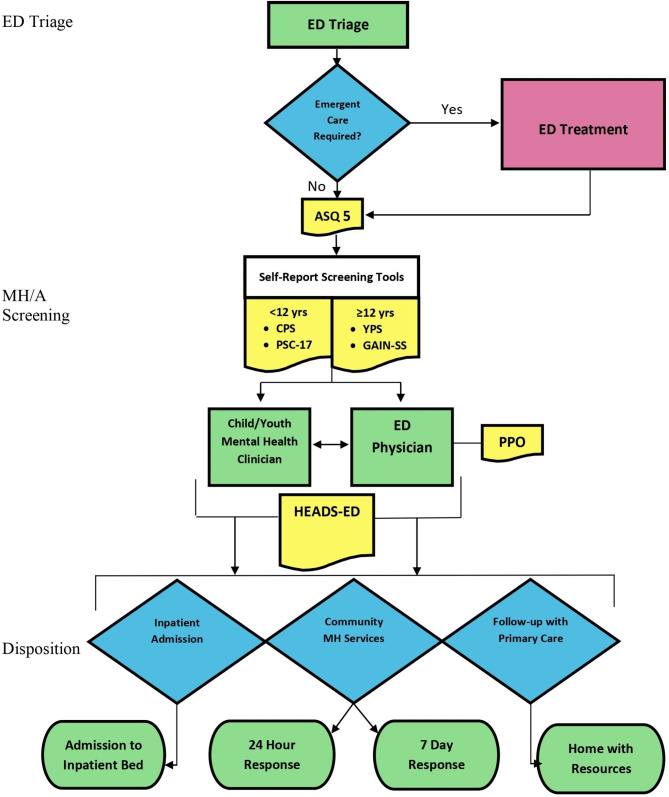
Emergency departments (EDs) are often the first access point for children and youth seeking mental health (MH) and addiction care. However, many EDs are unprepared to manage large volumes of pediatric MH patients. In addition, the fragmented Canadian MH system is challenged in connecting youth seen in the ED for follow-up community services. A provincial Emergency Department Mental Health Clinical Pathway (EDMHCP) for children and youth presenting to the ED with MH concerns was developed to address these challenges. The objective of the current study was to determine if EDMHCP implementation resulted in: (1) pathway use, (2) more patients discharged with MH recommendations, (3) MH service recommendations that aligned with patients' risk assessments, and (4) changes in service outcomes, including ED length of stay (LOS), revisits, and admissions/transfers.
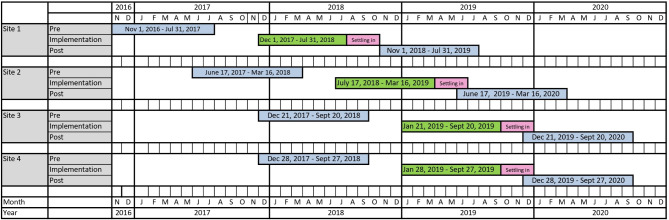
We implemented the pathway at four ED sites from 2018 to 2019 using the Theoretical Domains Framework to develop a tailored strategy at each site. We conducted chart reviews retrospectively in 2017-2018 (pre-implementation) and prospectively in 2019-2020 (post-implementation). Non-parametric tests examined differences in service outcomes between the implementation periods.
Pathway use varied widely across sites, ranging from 3.1% at site 4 to 83.0% at the lead site (site 2). More referrals to community MH agencies (p <.001) were made at discharge during post-implementation at the lead site compared to pre-implementation, and mixed results were obtained regarding whether clinicians' risk assessments aligned with MH service recommendations. LOS significantly increased at the lead site (p <.001) and non-lead sites (sites 1, 3, 4; p =.02) between pre- and post-implementation. Revisits and admissions/transfers did not change significantly at any site.
Implementation was partially successful at the lead site, showing high pathway use and greater referrals to community MH agencies. These findings emphasize the complexity of implementing pathways in various ED settings. Successful implementation requires integration into existing workflows.
ClinicalTrials.gov (NCT02590302). Registered on 29 October 2015.
急诊科往往是儿童和青少年寻求心理健康(MH)及成瘾治疗的首个接入点。然而,许多急诊科并未做好应对大量儿科心理健康患者的准备。此外,加拿大碎片化的心理健康系统在为急诊科就诊的青少年衔接后续社区服务方面面临挑战。针对因心理健康问题前往急诊科就诊的儿童和青少年,制定了省级急诊科心理健康临床路径(EDMHCP),以应对这些挑战。本研究的目的是确定EDMHCP的实施是否带来了以下结果:(1)路径使用情况;(2)更多患者出院时带有心理健康建议;(3)与患者风险评估相符的心理健康服务建议;(4)服务结果的变化,包括急诊科住院时间(LOS)、复诊情况以及入院/转院情况。
我们于2018年至2019年在四个急诊科实施了该路径,运用理论领域框架为每个地点制定了量身定制的策略。我们在2017 - 2018年(实施前)进行了回顾性病历审查,并在2019 - 2020年(实施后)进行了前瞻性审查。非参数检验用于检查实施期间服务结果的差异。
各地点的路径使用情况差异很大,从第4个地点的3.1%到主要地点(第2个地点)的83.0%不等。与实施前相比,主要地点在实施后出院时转介至社区心理健康机构的情况更多(p <.001),关于临床医生的风险评估是否与心理健康服务建议相符,结果不一。实施前后,主要地点(p <.001)和非主要地点(第1、3、4个地点;p =.02)的住院时间显著增加。任何地点的复诊情况以及入院/转院情况均未出现显著变化。
主要地点的实施部分成功,路径使用率高,转介至社区心理健康机构的情况更多。这些发现强调了在不同急诊科环境中实施路径的复杂性。成功实施需要融入现有的工作流程。
ClinicalTrials.gov(NCT02590302)。于2015年10月29日注册。