Zhou Yidan, Hu Jingjing
Department of Emergency Medicine, Hangzhou Third People's Hospital, Hangzhou, China.
BMC Infect Dis. 2025 Apr 9;25(1):486. doi: 10.1186/s12879-025-10880-z.
Sepsis-associated acute kidney injury (SA-AKI) significantly impacts global health. Early identification of SA-AKI patients at inflammatory and immune risk, followed by timely interventions, is critical for improving outcomes. The pan-immune-inflammation value (PIV) reflects systemic inflammation and immune status. However, its prognostic value in SA-AKI remains unexplored.
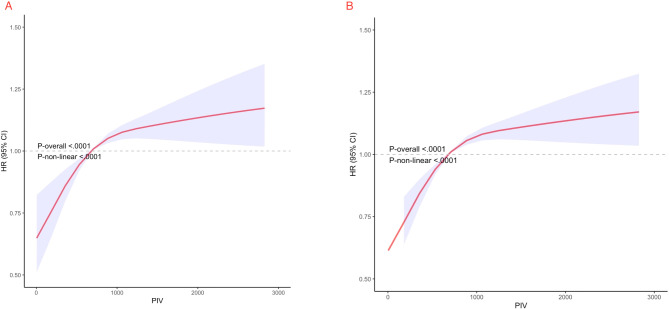
This retrospective cohort study analyzed SA-AKI patients in the MIMIC-IV database. Cox regression assessed the association between PIV and mortality, while restricted cubic spline (RCS) regression explored the relationship between PIV and 30-day and 365-day mortality.
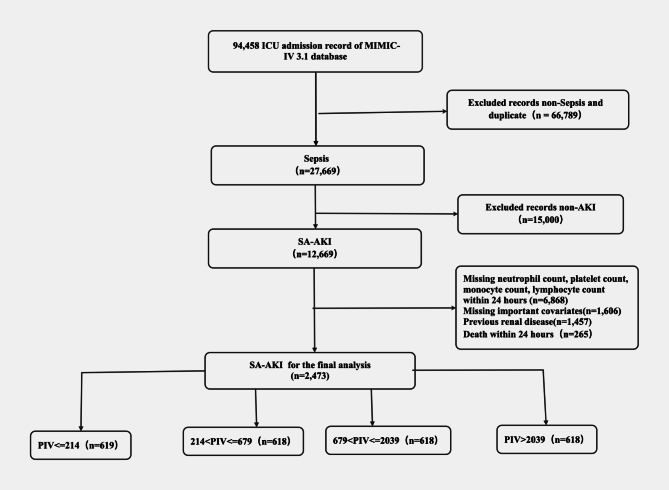
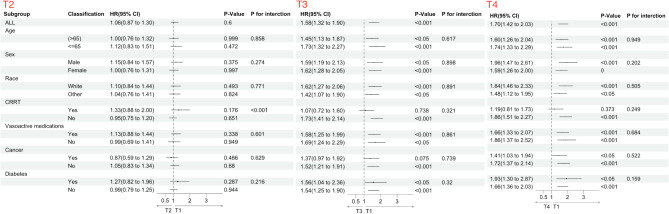
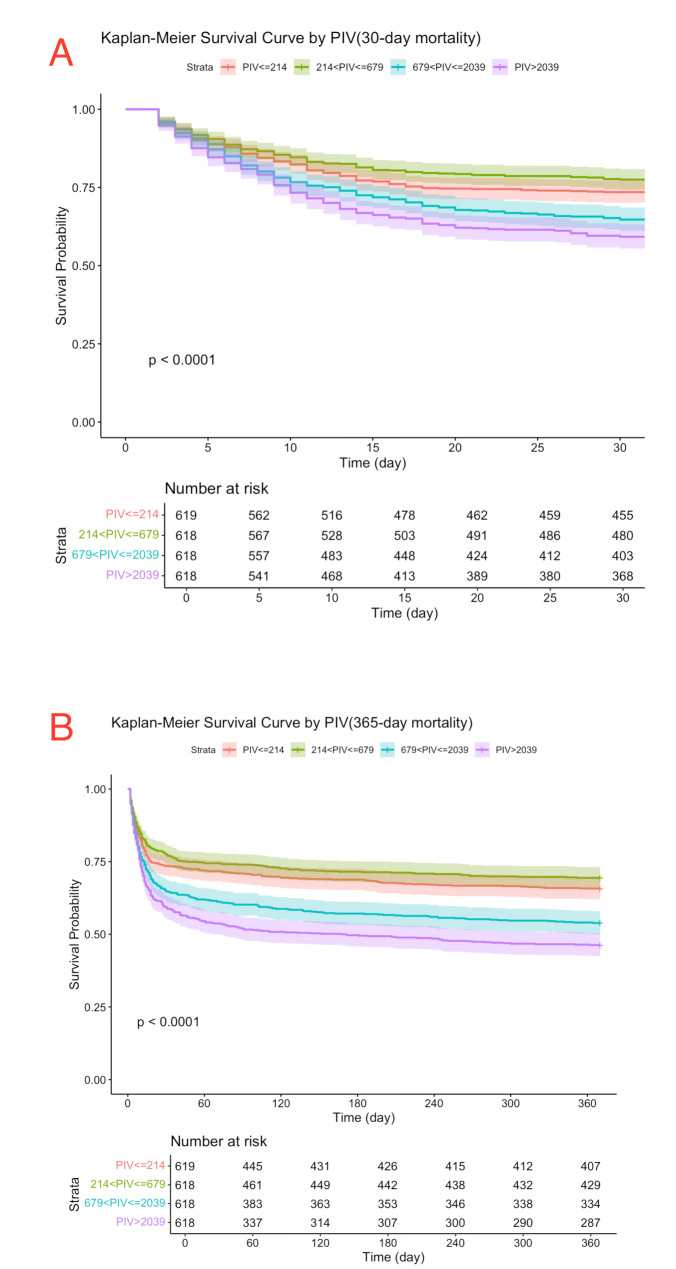
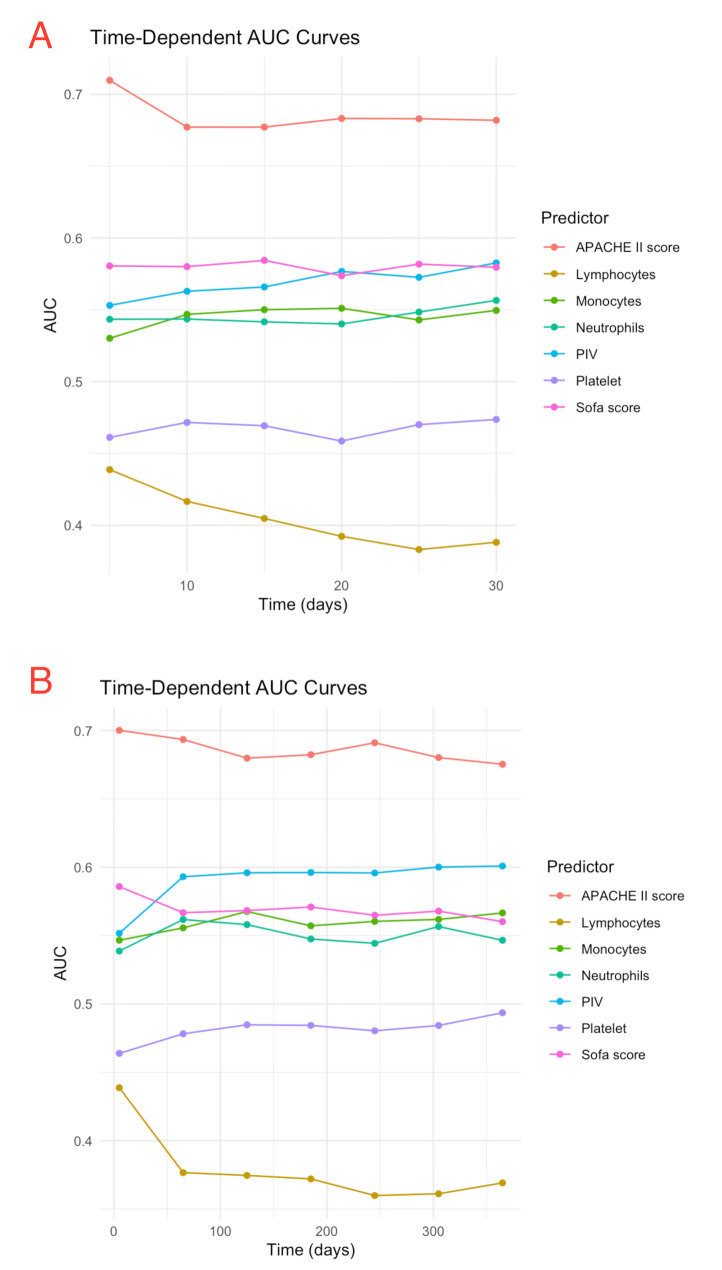
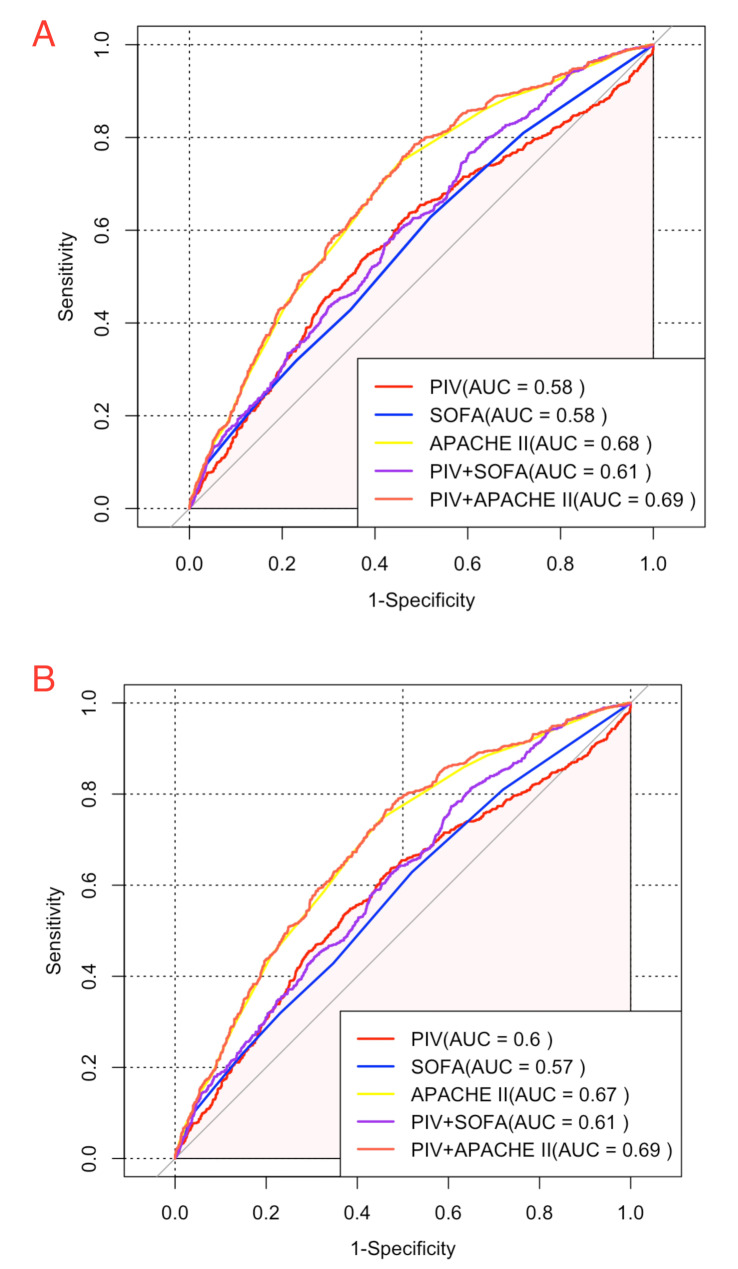
A total of 2,473 SA-AKI patients in our study were categorized into PIV quartiles: T1 (≤ 214), T2 (214-679), T3 (679-2,039), and T4 (> 2,039). PIV showed a nonlinear association with mortality. Higher PIV quartiles were linked to increased mortality, with 30-day rates of 26%, 22%, 35%, and 41% (P < 0.001) and 365-day mortality rates of 34%, 31%, 46%, and 54% (P < 0.001). Adjusted hazard ratios (HR) for 30-day mortality across quartiles were 1.00 (reference), 1.04(0.82, 1.31), 1.54 (1.25, 1.9), and 1.62 (1.32, 1.98), respectively. For 365-day mortality, the HR and 95% CI were 1.00 (reference), 1.06 (0.87, 1.30), 1.58 (1.32, 1.90), and 1.70 (1.42, 2.03). After adding PIV to SOFA score, the integrated discrimination improvement (IDI) for 30-day mortality was 0.005, and the net reclassification improvement (NRI) was 0.103. For 365-day mortality, the IDI was 0.009, and the NRI was 0.124. Regarding the APACHE II score, the IDI for 30-day mortality was 0.003, and the NRI was 0.081. For 365-day mortality, the IDI was 0.006, and the NRI was 0.107.
Elevated PIV independently predicts both short- and long-term adverse outcomes in SA-AKI patients. Incorporating PIV into established critical illness prediction models, such as SOFA and APACHE II, enhances their prognostic accuracy.
脓毒症相关急性肾损伤(SA-AKI)对全球健康有重大影响。早期识别处于炎症和免疫风险的SA-AKI患者,并及时进行干预,对于改善预后至关重要。全免疫炎症值(PIV)反映全身炎症和免疫状态。然而,其在SA-AKI中的预后价值仍未得到探索。
这项回顾性队列研究分析了多中心重症医学信息数据库第四版(MIMIC-IV)中的SA-AKI患者。Cox回归评估PIV与死亡率之间的关联,而受限立方样条(RCS)回归探讨PIV与30天和365天死亡率之间的关系。
我们研究中的2473例SA-AKI患者被分为PIV四分位数:T1(≤214)、T2(214-679)、T3(679-2039)和T4(>2039)。PIV与死亡率呈非线性关联。较高的PIV四分位数与死亡率增加相关,30天死亡率分别为26%、22%、35%和41%(P<0.001),365天死亡率分别为34%、31%、46%和54%(P<0.001)。各四分位数30天死亡率的调整后风险比(HR)分别为1.00(参考值)、1.04(0.82,1.31)、1.54(1.25,1.9)和1.62(1.32,1.98)。对于365天死亡率,HR和95%可信区间分别为1.00(参考值)、1.06(0.87,1.30)、1.58(1.32,1.90)和1.70(1.42,2.03)。将PIV添加到序贯器官衰竭评估(SOFA)评分中后,30天死亡率的综合判别改善(IDI)为0.005,净重新分类改善(NRI)为0.103。对于365天死亡率,IDI为0.009,NRI为0.124。关于急性生理与慢性健康状况评分系统II(APACHE II)评分,30天死亡率的IDI为0.003,NRI为0.081。对于365天死亡率,IDI为0.006,NRI为0.107。
PIV升高独立预测SA-AKI患者的短期和长期不良结局。将PIV纳入既定的危重病预测模型,如SOFA和APACHE II,可提高其预后准确性。