Bottomley Christian, Kamau Alice, Awori Juliet O, Driscoll Amanda J, Park Daniel E, Sow Samba O, Tapia Milagritos D, Kotloff Karen L, Ebruke Bernard E, Antonio Martin, Howie Stephen R C, Hayes Richard J, Scott J Anthony G
International Statistics and Epidemiology Group, London School of Hygiene & Tropical Medicine, London, United Kingdom.
Department of Infectious Disease Epidemiology and International Health, London School of Hygiene & Tropical Medicine, London, United Kingdom.
Int J Epidemiol. 2025 Feb 16;54(2). doi: 10.1093/ije/dyaf040.
The World Health Organization (WHO) clinical case definitions for pneumonia were designed to prioritize sensitivity over specificity. In sub-Saharan Africa, the disease that is most likely to be misclassified as pneumonia is Plasmodium falciparum malaria.
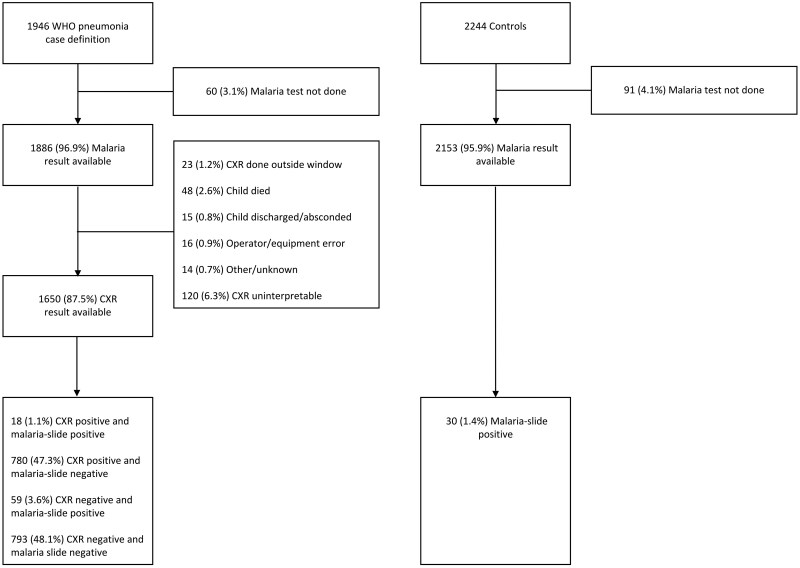
By using chest X-ray positivity as an indicator for pneumonia, we estimated the extent of pneumonia misclassification due to malaria in the Pneumonia Etiology Research for Child Health (PERCH) study. Additionally, we developed a simple model to predict the proportion of pneumonia cases as defined by the WHO that could be attributed to malaria in settings with varying levels of malaria parasitaemia prevalence.
In the PERCH study, the prevalence of malaria parasitaemia was low (4.7% among WHO pneumonia cases and 1.4% among controls) and we estimate that only 2.5% of WHO pneumonia cases were misclassified. However, when assuming a prevalence of malaria parasitaemia of 24%, corresponding to the average for malaria-endemic areas in Africa, we estimate that 28% of WHO pneumonia cases are misclassified. Among malaria-slide-positive WHO pneumonia cases in PERCH, lower chest wall indrawing [adjusted odds ratio (aOR) =18.1, 95% confidence interval (95% CI): 1.9, 175.8, P = 0.012], crackles on chest auscultation (aOR = 13.1, 95% CI: 1.4, 127.4, P = 0.027), and nasal flaring (aOR = 5.9, 95% CI: 1.1, 32.8, P = 0.041) were associated with chest X-ray positivity.
In settings that are typical of sub-Saharan Africa, we predict that one-quarter of WHO-defined pneumonia cases are malaria rather than pneumonia. Among children with WHO pneumonia who also test positive for malaria parasitaemia, clinical features that favour pneumonia include lower chest wall indrawing, nasal flaring, and crackles on chest auscultation.
世界卫生组织(WHO)的肺炎临床病例定义旨在优先考虑敏感性而非特异性。在撒哈拉以南非洲,最有可能被误诊为肺炎的疾病是恶性疟原虫疟疾。
在儿童健康肺炎病因研究(PERCH)中,我们以胸部X线阳性作为肺炎指标,估计了疟疾导致的肺炎误诊程度。此外,我们开发了一个简单模型,以预测在疟疾寄生虫血症患病率不同的环境中,WHO定义的肺炎病例中可归因于疟疾的比例。
在PERCH研究中,疟疾寄生虫血症患病率较低(WHO肺炎病例中为4.7%,对照组中为1.4%),我们估计只有2.5%的WHO肺炎病例被误诊。然而,假设疟疾寄生虫血症患病率为24%(对应于非洲疟疾流行地区的平均水平),我们估计28%的WHO肺炎病例被误诊。在PERCH中疟疾涂片阳性的WHO肺炎病例中,下胸壁凹陷(调整优势比[aOR]=18.1,95%置信区间[95%CI]:1.9,175.8,P=0.012)、胸部听诊有啰音(aOR=13.1,95%CI:1.4,127.4,P=0.027)和鼻翼扇动(aOR=5.9,95%CI:1.1,32.8,P=0.041)与胸部X线阳性相关。
在撒哈拉以南非洲的典型环境中,我们预测WHO定义的肺炎病例中有四分之一是疟疾而非肺炎。在WHO诊断为肺炎且疟疾寄生虫血症检测也呈阳性的儿童中,提示肺炎的临床特征包括下胸壁凹陷、鼻翼扇动和胸部听诊有啰音。