Zile Michael R, Abraham William T, Stevenson Lynne W, Costanzo Maria Rosa, Angermann Christiane E, Mehra Mandeep R, Desai Akshay S, Ducharme Anique, Johnson Nessa, Henderson John, Lindenfeld JoAnn
Medical University of South Carolina, RJH Department of Veterans Affairs Health Care System, Charleston (M.R.Z.).
Ohio State University, Wexner Medical Center, Columbus (W.T.A.).
Circ Heart Fail. 2025 Jun;18(6):e012754. doi: 10.1161/CIRCHEARTFAILURE.124.012754. Epub 2025 Apr 14.
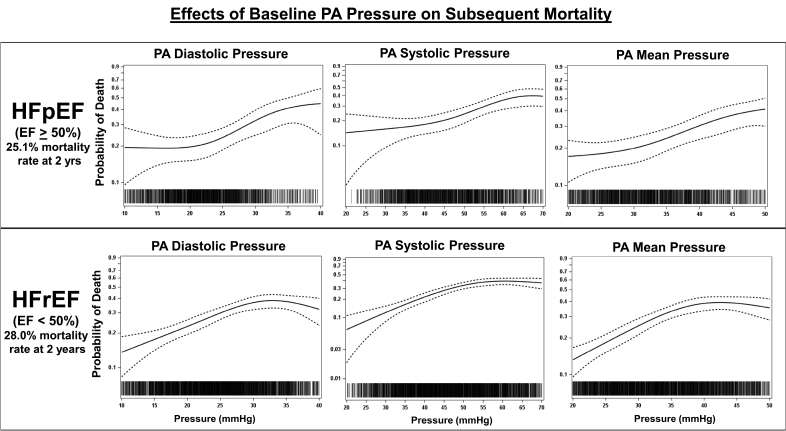
Hemodynamically guided management of patients with chronic heart failure (HF), using a remote, ambulatory pulmonary artery (PA) pressure monitor, has been shown to reduce mortality and morbidity. These improved outcomes were associated with a reduction in PA pressure. However, several pivotal questions remain unanswered: do systolic, diastolic, or mean PA pressures each predict all-cause mortality? Do PA pressures predict mortality across the ejection fraction (EF) spectrum? Do increases or decreases in PA pressure over time predict increases or decreases in mortality?
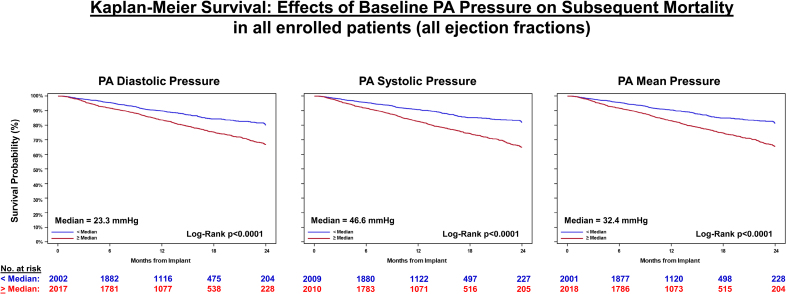
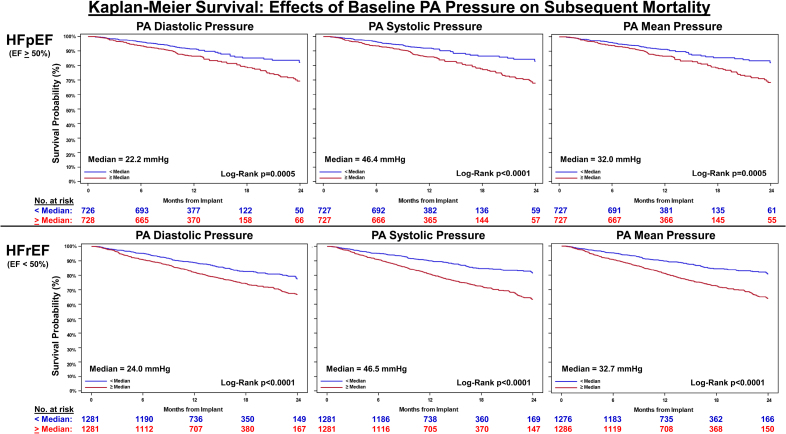
Retrospective analyses of data from CHAMPION (CardioMEMS Heart Sensor Allows Monitoring of Pressure to Improve Outcomes in NYHA Class III Heart Failure Patients; n=550), GUIDE-HF (Hemodynamic-GUIDEed management of Heart Failure; n=2358), US PAS (CardioMEMS HF System Post Approval Study; n=1200), and MEMS-HF (CardioMEMS Monitoring Study for Heart Failure; n=234) were performed, including all enrolled patients regardless of treatment assignments (Total N=4342). PA systolic, PA diastolic, and PA mean pressures were examined in patients with HF and reduced EF (<50%, n=2562) and preserved EF (≥50%, n=1454). Baseline pressure (averaged over 14 days after implantation) and change in pressure (increase/decrease/no change) from baseline to 6 months (averaged over 14 days just before the 6-month time point) were related to all-cause mortality over a 2-year follow-up period.
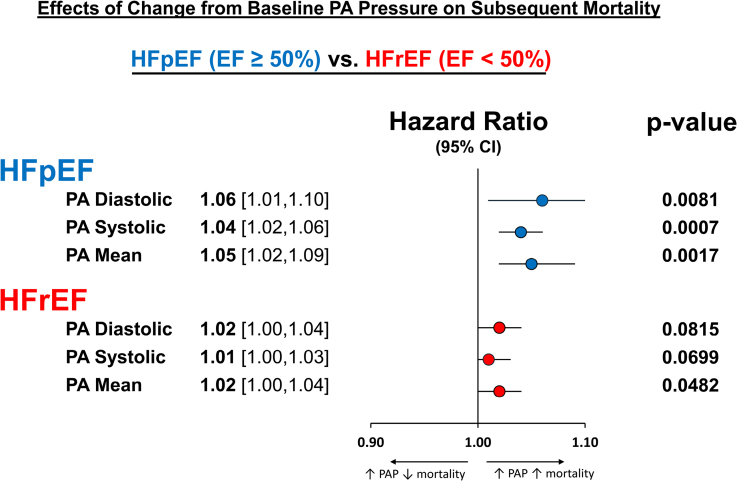
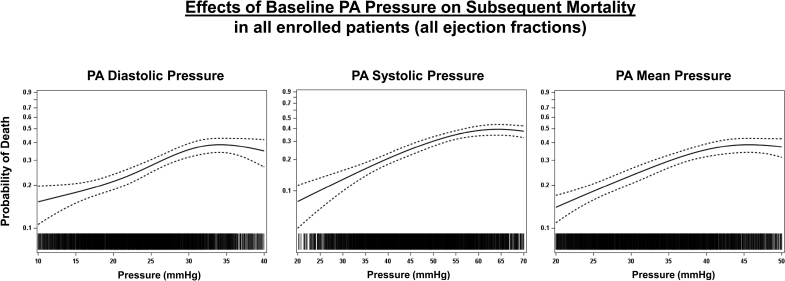
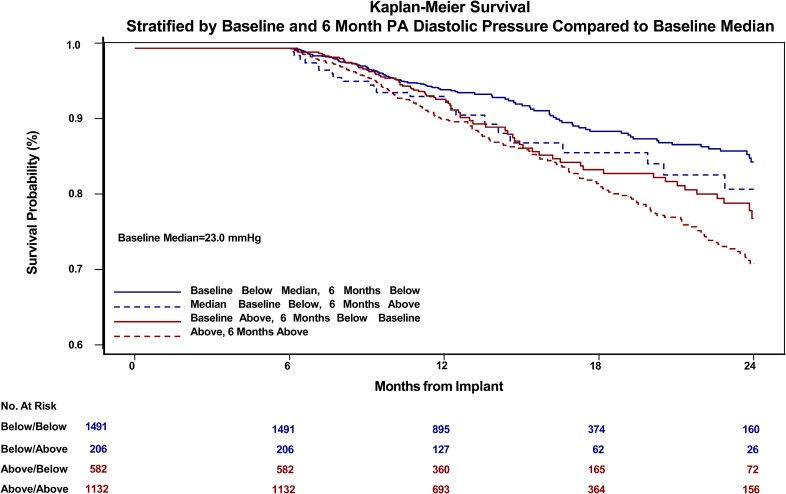
Baseline PA diastolic, independent of other covariates, was a significant predictor of mortality (hazard ratio, 1.04 [95% CI, 1.03-1.05]; <0.0001). Change in PA diastolic from baseline to 6 months (assessed as a continuous variable) was an independent predictor of mortality after 6 months (landmark analysis; hazard ratio, 1.03 [95% CI, 1.01-1.05]; =0.0042). Change in PA diastolic from baseline to 6 months(assessed as a categorical variable) decrease or increase of >2 mm Hg compared with no change predicted a 14.7% decrease and 26.7% increase in mortality, respectively (=0.0237). PA systolic and PA mean pressures in both HF with reduced EF and HF with preserved EF patients, for both baseline and change from baseline to 6 months, were also predictive of all-cause mortality.
Baseline PAP (systolic, diastolic, and mean) and change in PAP (systolic, diastolic, and mean) from baseline to 6 months were independent predictors of 2-year mortality in patients with chronic HF in both preserved and reduced EF.
URL: https://www.clinicaltrials.gov; Unique identifiers: CHAMPION, NCT00531661; GUIDE-HF, NCT03387813; USPAS, NCT02279888; MEMS-HF, NCT02693691.
使用远程动态肺动脉(PA)压力监测仪对慢性心力衰竭(HF)患者进行血流动力学指导管理,已显示可降低死亡率和发病率。这些改善的结果与PA压力降低有关。然而,几个关键问题仍未得到解答:收缩期、舒张期或平均PA压力是否均可预测全因死亡率?PA压力是否能在整个射血分数(EF)范围内预测死亡率?随时间推移PA压力的升高或降低是否能预测死亡率的升高或降低?
对CHAMPION(心脏MEMS传感器允许监测压力以改善纽约心脏协会III级心力衰竭患者的结局;n = 550)、GUIDE-HF(心力衰竭的血流动力学指导管理;n = 2358)、美国PAS(心脏MEMS HF系统批准后研究;n = 1200)和MEMS-HF(心力衰竭的心脏MEMS监测研究;n = 234)的数据进行回顾性分析,纳入所有登记患者,无论其治疗分配情况如何(总计N = 4342)。在射血分数降低(<50%,n = 2562)和射血分数保留(≥50%,n = 1454)的HF患者中检查PA收缩压、PA舒张压和PA平均压。将基线压力(植入后14天的平均值)以及从基线到6个月时压力的变化(升高/降低/无变化)(6个月时间点前14天的平均值)与2年随访期内的全因死亡率相关联。
独立于其他协变量,基线PA舒张压是死亡率的显著预测因素(风险比,1.04 [95% CI,1.03 - 1.05];P < 0.0001)。从基线到6个月时PA舒张压的变化(作为连续变量评估)是6个月后死亡率的独立预测因素(标志性分析;风险比,1.03 [95% CI,1.01 - 1.05];P = 0.0042)。从基线到6个月时PA舒张压的变化(作为分类变量评估),与无变化相比,降低或升高>2 mmHg分别预测死亡率降低14.7%和升高26.7%(P = 0.0237)。在射血分数降低的HF患者和射血分数保留的HF患者中,基线时以及从基线到6个月时的PA收缩压和PA平均压也可预测全因死亡率。
基线肺动脉压(收缩压、舒张压和平均压)以及从基线到6个月时肺动脉压的变化(收缩压、舒张压和平均压)是射血分数保留和降低的慢性HF患者2年死亡率的独立预测因素。