Krisai Philipp, Eberl Magdalena, Coslovsky Michael, Rodondi Nicolas, Chocano-Bedoya Patricia, Aeschbacher Stefanie, Balasundaram Sujeena, Rolny Vinzent, Kobza Richard, Moschovitis Giorgio, Rigamonti Elia, Beer Jürg H, Müller Andreas, Reichlin Tobias, Conen David, Osswald Stefan, Bonati Leo H, Kühne Michael
Department of Cardiology and Cardiovascular Research Institute Basel, University Hospital Basel, University of Basel, Petersgraben 4, 4031, Basel, Switzerland.
Roche Diagnostics GmbH, Penzberg, Germany.
Sci Rep. 2025 Apr 15;15(1):12921. doi: 10.1038/s41598-025-89800-9.
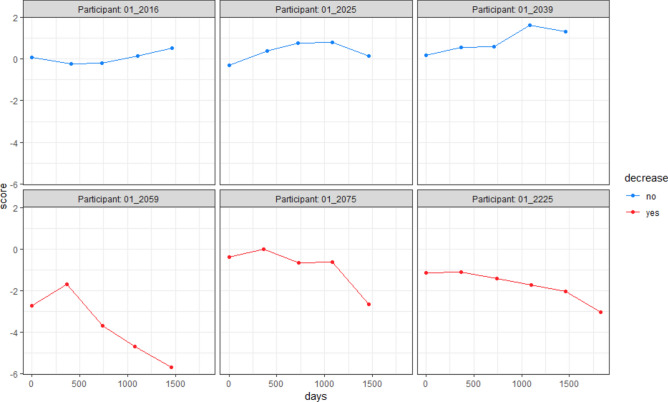
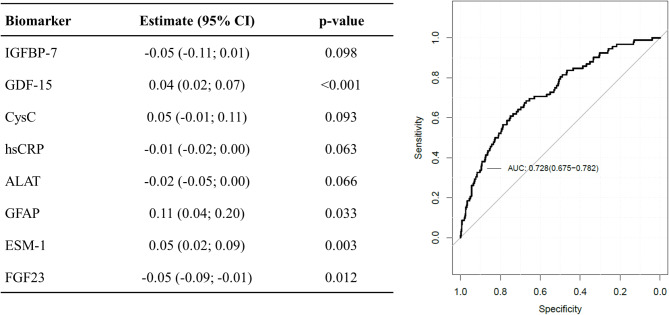
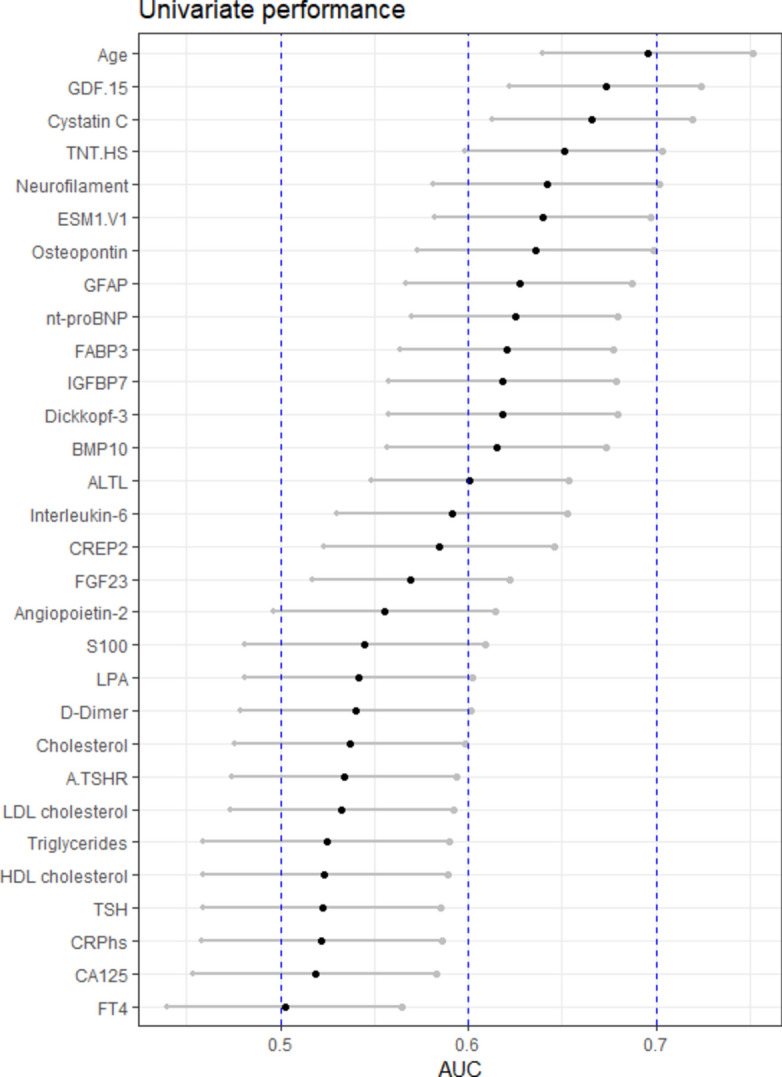
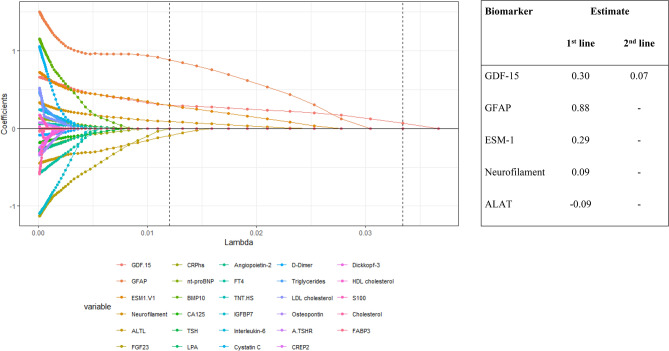
We investigated associations of a broad biomarker panel with cognitive decline in atrial fibrillation (AF) patients to characterize possible mechanisms. We enrolled 1440 AF patients with available baseline biomarkers and cognitive testing by the Montreal Cognitive assessment (MoCA) score at inclusion and at ≥ 2 yearly follow-ups. We investigated the associations of biomarkers with cognitive decline in univariate logistic regression models, LASSO regression analysis and built a combined model. Mean age was 72 years, 75% male, 47% paroxysmal AF. Over 4 years, 93 patients (6.5%) had cognitive decline. These patients had more often permanent AF (32.3 vs 21.5%, p = 0.007) and more often a history stroke (23.7 vs 11.2%, p < 0.001), but similar baseline MoCA scores (24.9 vs 25.3 points, p = 0.22) and anticoagulation rates (93.5 vs 89.5%, p = 0.29). The three biomarkers with the highest univariate AUC for cognitive decline were GDF-15 (0.67 [0.62-0.72]), Cystatin C (0.67 [0.61-0.72]) and high-sensitivity Troponin T (hs-TnT) (0.65 [0.60-0.70]). In LASSO regression analysis, the best cross validation included GDF-15, GFAP, ESM-1, NfL and ALAT. The combined prediction model with the highest AUC of 0.73 (0.68-0.78) included IGFBP-7, GDF-15, Cystatin C, hsCRP, ALAT, GFAP, ESM-1 and FGF23. Over 4 years, 6.5% of AF patients had cognitive decline despite a high rate of anticoagulation. Inflammation, neuronal damage, and increased amyloid-beta might be important non-ischemic mechanisms of cognitive decline in AF patients.
我们研究了一组广泛的生物标志物与心房颤动(AF)患者认知功能下降之间的关联,以阐明可能的机制。我们纳入了1440例AF患者,这些患者在入组时以及≥2年的年度随访时均有可用的基线生物标志物,并通过蒙特利尔认知评估(MoCA)评分进行认知测试。我们在单变量逻辑回归模型、LASSO回归分析中研究了生物标志物与认知功能下降之间的关联,并建立了一个综合模型。平均年龄为72岁,75%为男性,47%为阵发性AF。在4年多的时间里,93例患者(6.5%)出现了认知功能下降。这些患者永久性AF的发生率更高(32.3%对21.5%,p = 0.007),中风病史的发生率也更高(23.7%对11.2%,p < 0.001),但基线MoCA评分相似(24.9分对25.3分,p = 0.22),抗凝率也相似(93.5%对89.5%,p = 0.29)。单变量分析中对认知功能下降AUC最高的三种生物标志物是生长分化因子15(GDF-15)(0.67[0.62 - 0.72])、胱抑素C(0.67[0.61 - 0.72])和高敏肌钙蛋白T(hs-TnT)(0.65[0.60 - 0.70])。在LASSO回归分析中,最佳交叉验证纳入了GDF-15、胶质纤维酸性蛋白(GFAP)、内皮抑素(ESM-1)、神经丝轻链(NfL)和丙氨酸氨基转移酶(ALAT)。AUC最高为0.73(0.68 - 0.78)的联合预测模型纳入了胰岛素样生长因子结合蛋白7(IGFBP-7)、GDF-15、胱抑素C、高敏C反应蛋白(hsCRP)、ALAT、GFAP、ESM-1和成纤维细胞生长因子23(FGF23)。在4年多的时间里,尽管抗凝率很高,但仍有6.5%的AF患者出现了认知功能下降。炎症、神经元损伤和β淀粉样蛋白增加可能是AF患者认知功能下降的重要非缺血机制。