Mancuso Noah, Michaels Jenna, Browne Erica N, Maragh-Bass Allysha C, Stocks Jacob B, Soberano Zachary R, Bond C Lily, Yigit Ibrahim, Comello Maria Leonora G, Larsen Margo Adams, Muessig Kathryn E, Pettifor Audrey, Hightow-Weidman Lisa B, Budhwani Henna, Stoner Marie C D
Women's Global Health Imperative, Research Triangle Institute (RTI) International, 3040 East Cornwallis Road, Research Triangle Park, NC, 27709, United States, 1 9195416000.
Department of Epidemiology, Emory University, Atlanta, GA, United States.
JMIR Public Health Surveill. 2025 Apr 16;11:e67370. doi: 10.2196/67370.
Negative attitudes toward vaccines and suboptimal vaccination rates among African American and Black (Black) Americans have been well documented, due to a history of medical racism and human rights violations in the United States. However, digital health interventions (DHI) have been shown to address racial disparities in several health outcomes, such as cardiovascular disease, HIV, and maternal health. The Tough Talks COVID (TT-C) study was a randomized controlled trial of a DHI designed to empower Black young adults in the United States South to make informed, autonomous decisions about COVID-19 vaccine uptake by addressing structural barriers and misinformation about vaccines.
Our objective was to identify subgroups of Black young adults with various vaccine attitudes at baseline and determine the subgroups for which the TT-C DHI was most impactful.
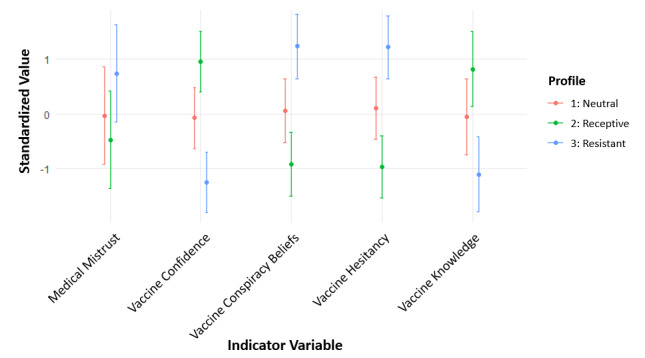
Black young adults aged 18-29 years in Alabama, Georgia, and North Carolina who were unvaccinated or insufficiently vaccinated against COVID-19 completed three online surveys over three months (N=360). Latent profile analysis was used to identify subgroups based on general vaccine attitudes at baseline, including hesitancy, confidence, knowledge, conspiracy beliefs, and mistrust. Logistic regression was used to examine the associations between latent profiles and vaccine uptake, and linear regression was used to examine changes in vaccine attitudes at three months post-randomization. Modification of the TT-C DHI's effects was assessed by latent profiles.
Three latent profiles emerged: vaccine-receptive (n=124), vaccine-neutral (n=155), and vaccine-resistant (n=81). Political affiliation, income, social support, and recent flu vaccination differed significantly between the three subgroups (P<.05). Vaccine uptake was not significantly different by subgroup, and the TTC-DHI did not have differing effects on uptake across subgroups. However, the DHI had the strongest effect-with statistically significant measures of association (P<.05) and interaction P values (P<.10)-among the baseline vaccine-resistant and vaccine-neutral subgroups compared to the vaccine-receptive subgroups at three months in improving vaccine hesitancy, confidence, and conspiracy beliefs at three months: vaccine-resistant difference: -0.40 (-0.76 to -0.37), 0.39 (0.02 to 0.75), and -0.47 (-0.86 to -0.09); vaccine neutral difference: -0.36 (-0.52 to -0.19), 0.35 (0.18 to 0.51), and -0.24 (-0.44 to -0.03). The DHI had no effects on these outcomes among the vaccine-receptive subgroup.
Our findings revealed subgroups of Black young adults in the United States South with different vaccination attitudes, for which the TT-C intervention had differing effects. Black young adults who are vaccine-resistant or vaccine-neutral may experience larger gains from a digital vaccine intervention. Future work aimed at improving vaccination outcomes could target these populations to maximize resource efficiency and drive the greatest improvements in vaccine outcomes.
由于美国存在医疗种族主义和侵犯人权的历史,非裔美国人和黑人对疫苗的负面态度以及次优的疫苗接种率已有充分记录。然而,数字健康干预措施(DHI)已被证明可解决心血管疾病、艾滋病毒和孕产妇健康等多种健康结果方面的种族差异。“艰难对话新冠”(TT-C)研究是一项针对DHI的随机对照试验,旨在通过消除结构障碍和有关疫苗的错误信息,使美国南部的黑人青年能够就新冠疫苗接种做出明智、自主的决定。
我们的目的是确定基线时具有不同疫苗态度的黑人青年亚组,并确定TT-C DHI对其影响最大的亚组。
阿拉巴马州、佐治亚州和北卡罗来纳州18至29岁未接种或未充分接种新冠疫苗的黑人青年在三个月内完成了三项在线调查(N = 360)。潜在类别分析用于根据基线时的一般疫苗态度确定亚组,包括犹豫、信心、知识、阴谋论信念和不信任。逻辑回归用于检验潜在类别与疫苗接种之间的关联,线性回归用于检验随机分组后三个月疫苗态度的变化。通过潜在类别评估TT-C DHI效果的改变。
出现了三个潜在类别:疫苗接受型(n = 124)、疫苗中立型(n = 155)和疫苗抗拒型(n = 81)。三个亚组之间的政治派别、收入、社会支持和近期流感疫苗接种情况存在显著差异(P <.05)。亚组之间的疫苗接种率无显著差异,TTC-DHI对各亚组的接种效果也无差异。然而,与疫苗接受型亚组相比,DHI在三个月时对基线时疫苗抗拒型和疫苗中立型亚组在改善疫苗犹豫、信心和阴谋论信念方面具有最强的效果——具有统计学显著的关联度量(P <.05)和交互P值(P <.10):疫苗抗拒型差异:-0.40(-0.76至-0.37),0.39(0.02至0.75),和-0.47(-0.86至-0.09);疫苗中立型差异:-0.36(-0.52至-0.19),0.35(0.18至0.51),和-0.24(-0.44至-0.03)。DHI对疫苗接受型亚组的这些结果没有影响。
我们的研究结果揭示了美国南部具有不同疫苗接种态度的黑人青年亚组,TT-C干预对其有不同影响。疫苗抗拒型或疫苗中立型的黑人青年可能从数字疫苗干预中获得更大收益。未来旨在改善疫苗接种结果的工作可以针对这些人群,以最大限度地提高资源效率并推动疫苗结果的最大改善。