Myers Regina M, DiNofia Amanda M, Li Yimei, Diorio Caroline, Liu Hongyan, Wertheim Gerald, Fraietta Joseph A, Gonzalez Vanessa, Plesa Gabriela, Siegel Donald L, Iannone Emma, Shinehouse Laura, Brogdon Jennifer L, Taylor Clare, Jadlowsky Julie K, Hexner Elizabeth O, Engels Boris, Baniewicz Diane, Callahan Colleen, Ruella Marco, Aplenc Richard, Barz Leahy Allison, McClory Susan E, Rheingold Susan R, Wray Lisa, June Carl H, Maude Shannon L, Frey Noelle V, Grupp Stephan A
Division of Oncology, Center for Childhood Cancer Research, Children's Hospital of Philadelphia, Philadelphia, Pennsylvania, USA
Department of Pediatrics, University of Pennsylvania Perelman School of Medicine, Philadelphia, Pennsylvania, USA.
J Immunother Cancer. 2025 Apr 17;13(4):e011549. doi: 10.1136/jitc-2025-011549.
Relapse of B-cell acute lymphoblastic leukemia (B-ALL) with CD19-antigen loss after CD19-targeted chimeric antigen receptor (CAR) T-cell therapy has a dismal prognosis. Novel immunotherapeutic strategies for this patient population are urgently needed.
We tested a novel, fully human anti-CD22/4-1BB CAR T-cell construct, CART22-65s, in parallel phase I studies for pediatric and adult B-ALL. After lymphodepletion, CART22-65s was infused using a 3-day fractionated dosing scheme, allowing for omission of the second and third doses in cases of early cytokine release syndrome (CRS).
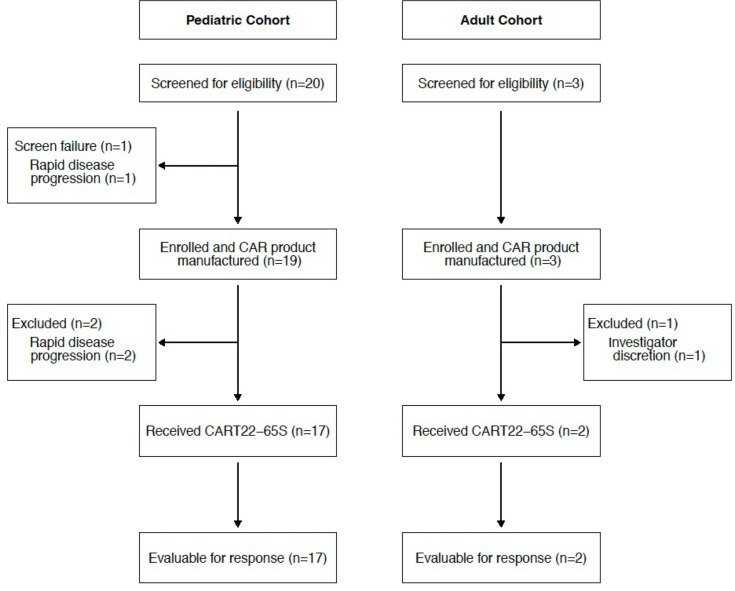
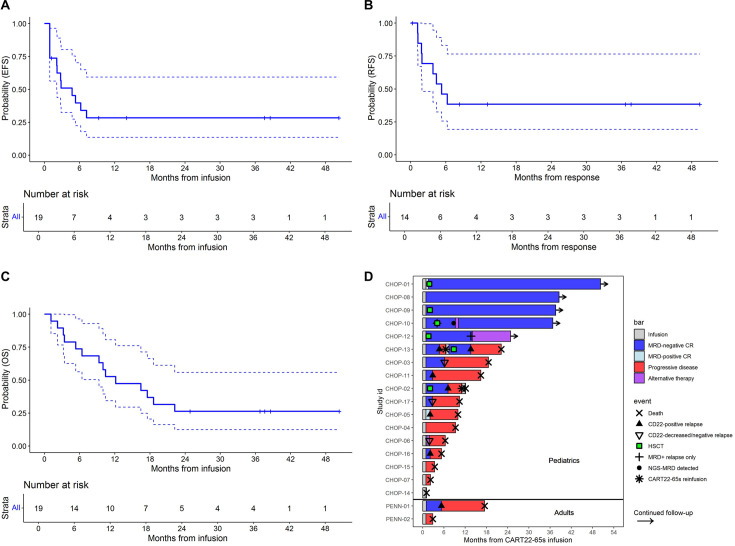
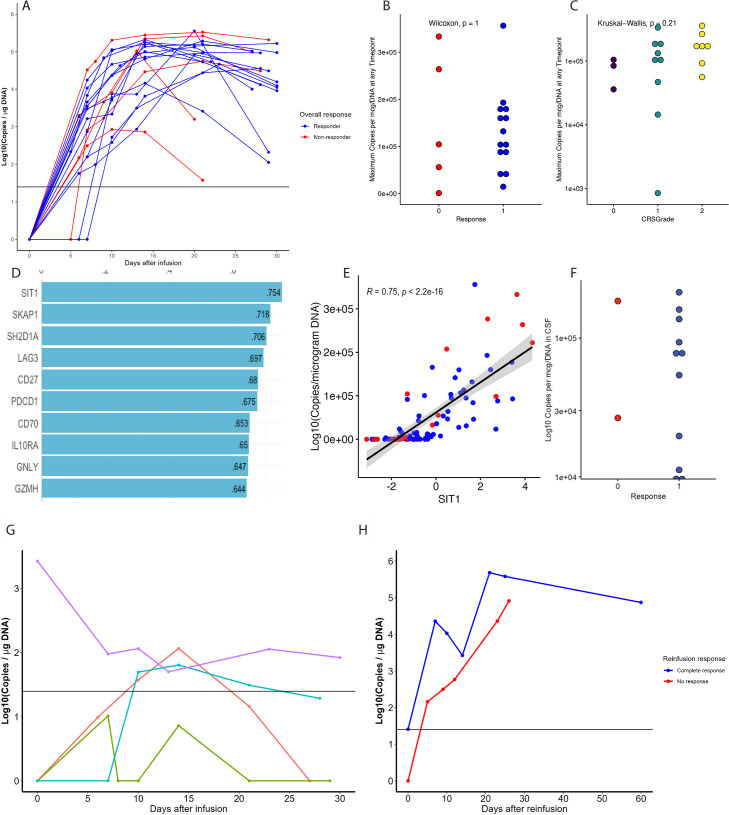
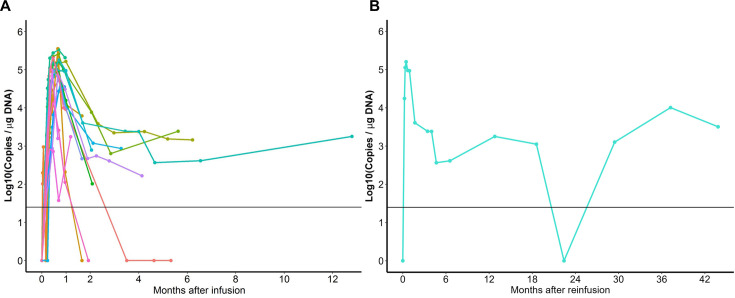
Twenty-two patients, all with relapse after prior CD19-directed immunotherapy, were enrolled. Of 19 infused patients (pediatric, n=17; adult, n=2), 14 (74%) achieved a complete remission (CR), including 4 of 6 (67%) patients refractory to prior inotuzumab. Five of 14 patients in a CR proceeded to consolidative hematopoietic cell transplantation (HCT). With a median follow-up of 38 months, the 12-month relapse-free survival rate was 38.4% (95% CI 19.3% to 76.5%) and overall survival rate was 52.6% (95% CI 34.3% to 80.6%). Two patients received additional CART22-65s treatments for subsequent CD22-positive relapses; one achieved another CR. All CRS (n=17, 89%) and neurotoxicity (n=4, 21%) events after initial infusion were grades 1-2. The only grade 3 CRS/neurotoxicity and the only high-grade immune effector cell-associated hemophagocytic lymphohistocytosis-like syndrome occurred in the retreatment setting. In vivo cellular kinetic data revealed robust CART22-65s proliferation by quantitative PCR peaking at a median of 20 days postinfusion, with the cells persisting out to month 42 in one patient who achieved a long-term remission with CART22-65s alone.
The favorable safety profile and high remission rates in exceedingly refractory B-ALL support the continued development of CART22-65s but also highlight the need to use the product in combination with HCT or other novel strategies.
NCT02650414 and NCT03620058.
在接受靶向CD19的嵌合抗原受体(CAR)T细胞治疗后,发生CD19抗原丢失的B细胞急性淋巴细胞白血病(B-ALL)复发,其预后很差。迫切需要针对这一患者群体的新型免疫治疗策略。
我们在针对儿童和成人B-ALL的平行I期研究中测试了一种新型的全人源抗CD22/4-1BB CAR T细胞构建体CART22-65s。在淋巴细胞清除后,采用3天分次给药方案输注CART22-65s,若出现早期细胞因子释放综合征(CRS),可省略第二剂和第三剂。
共纳入22例患者,均为先前接受CD19导向免疫治疗后复发的患者。在19例输注患者中(儿童17例,成人2例),14例(74%)实现完全缓解(CR),其中6例先前对吉妥珠单抗难治的患者中有4例(67%)实现缓解。14例CR患者中有5例接受了巩固性造血细胞移植(HCT)。中位随访38个月时,12个月无复发生存率为38.4%(95%CI 19.3%至76.5%),总生存率为52.6%(95%CI 34.3%至80.6%)。2例患者因后续CD22阳性复发接受了额外的CART22-65s治疗;1例再次实现CR。首次输注后的所有CRS(n = 17,89%)和神经毒性(n = 4,21%)事件均为1-2级。唯一的3级CRS/神经毒性事件和唯一的高级别免疫效应细胞相关噬血细胞性淋巴组织细胞增生症样综合征发生在再次治疗时。体内细胞动力学数据显示,通过定量PCR检测,CART22-65s在输注后中位20天达到增殖高峰,在1例仅接受CART22-65s治疗并实现长期缓解的患者中,细胞持续存在至42个月。
在极难治疗性B-ALL中,CART22-65s具有良好的安全性和高缓解率,这支持其继续研发,但也凸显了将该产品与HCT或其他新型策略联合使用的必要性。
NCT02650414和NCT03620058。