Fischerova D, Pinto P, Pesta M, Blasko M, Moruzzi M C, Testa A C, Franchi D, Chiappa V, Alcázar J L, Wiesnerova M, Cibula D, Valentin L
Gynecologic Oncology Centre, Department of Gynecology, Obstetrics and Neonatology, First Faculty of Medicine, Charles University and General University Hospital in Prague, Prague, Czech Republic.
Department of Gynecology, Portuguese Institute of Oncology Francisco Gentil, Lisbon, Portugal.
Ultrasound Obstet Gynecol. 2025 May;65(5):641-652. doi: 10.1002/uog.29208. Epub 2025 Apr 18.
To assess the ability, as well as factors affecting the ability, of ultrasound examiners with different levels of ultrasound experience to detect correctly infiltration of ovarian cancer in predefined anatomical locations, and to evaluate the inter-rater agreement regarding the presence or absence of cancer infiltration, using preacquired ultrasound videoclips obtained in a selected patient sample with a high prevalence of cancer spread.
This study forms part of the Imaging Study in Advanced ovArian Cancer multicenter observational study (NCT03808792). Ultrasound videoclips showing assessment of infiltration of ovarian cancer were obtained by the principal investigator (an ultrasound expert, who did not participate in rating) at 19 predefined anatomical sites in the abdomen and pelvis, including five sites that, if infiltrated, would indicate tumor non-resectability. For each site, there were 10 videoclips showing cancer infiltration and 10 showing no cancer infiltration. The reference standard was either findings at surgery with histological confirmation or response to chemotherapy. For statistical analysis, the 19 sites were grouped into four anatomical regions: pelvis, middle abdomen, upper abdomen and lymph nodes. The videoclips were assessed by raters comprising both senior gynecologists (mainly self-trained expert ultrasound examiners who perform preoperative ultrasound assessment of ovarian cancer spread almost daily) and gynecologists who had undergone a minimum of 6 months' supervised training in the preoperative ultrasound assessment of ovarian cancer spread in a gynecological oncology center. The raters were classified as highly experienced or less experienced based on annual individual caseload and the number of years that they had been performing ultrasound evaluation of ovarian cancer spread. Raters were aware that for each site there would be 10 videoclips with and 10 without cancer infiltration. Each rater independently classified every videoclip as showing or not showing cancer infiltration and rated the image quality (on a scale from 0 to 10) and their diagnostic confidence (on a scale from 0 to 10). A generalized linear mixed model with random effects was used to estimate which factors (including level of experience, image quality, diagnostic confidence and anatomical region) affected the likelihood of a correct classification of cancer infiltration. We assessed the observed percentage of videoclips classified correctly, the expected percentage of videoclips classified correctly based on the generalized linear mixed model and inter-rater agreement (reliability) in classifying anatomical sites as being infiltrated by cancer.
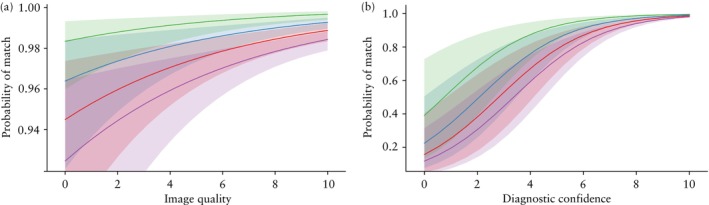
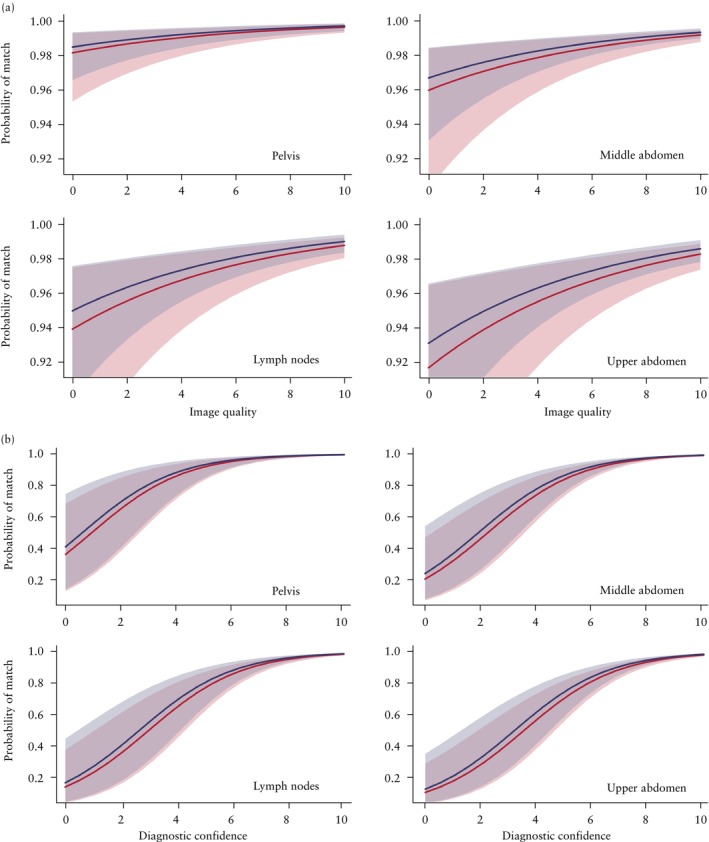
Twenty-five raters participated in the study, of whom 13 were highly experienced and 12 were less experienced. The observed percentage of correct classification of cancer infiltration ranged from 70% to 100% depending on rater and anatomical site, and the median percentage of correct classification for the 25 raters ranged from 90% to 100%. The probability of correct classification of all 380 videoclips ranged from 0.956 to 0.975 and was not affected by the rater's level of ultrasound experience. The likelihood of correct classification increased with increased image quality and diagnostic confidence and was affected by anatomical region. It was highest for sites in the pelvis, second highest for those in the middle abdomen, third highest for lymph nodes and lowest for sites in the upper abdomen. The inter-rater agreement of all 25 raters regarding the presence of cancer infiltration ranged from substantial (Fleiss kappa, 0.68 (95% CI, 0.66-0.71)) to very good (Fleiss kappa, 0.99 (95% CI, 0.97-1.00)) depending on the anatomical site. It was lowest for sites in the upper abdomen (Fleiss kappa, 0.68 (95% CI, 0.66-0.71) to 0.97 (95% CI, 0.94-0.99)) and highest for sites in the pelvis (Fleiss kappa, 0.94 (95% CI, 0.92-0.97) to 0.99 (95% CI, 0.97-1.00)).
Ultrasound examiners with different levels of ultrasound experience can classify correctly predefined anatomical sites as being infiltrated or not infiltrated by ovarian cancer based on video recordings obtained by an experienced ultrasound examiner, and the inter-rater agreement is substantial. The likelihood of correct classification as well as the inter-rater agreement is highest for sites in the pelvis and lowest for sites in the upper abdomen. However, owing to the study design, our results regarding diagnostic accuracy and inter-rater agreement are likely to be overoptimistic. © 2025 The Author(s). Ultrasound in Obstetrics & Gynecology published by John Wiley & Sons Ltd on behalf of International Society of Ultrasound in Obstetrics and Gynecology.
评估具有不同超声经验水平的超声检查人员正确检测卵巢癌在预定义解剖位置浸润的能力以及影响该能力的因素,并使用在癌症扩散患病率高的选定患者样本中预先获取的超声视频片段,评估检查人员之间关于癌症浸润存在与否的一致性。
本研究是晚期卵巢癌影像研究多中心观察性研究(NCT03808792)的一部分。主要研究者(一位超声专家,未参与评分)在腹部和盆腔的19个预定义解剖部位获取了显示卵巢癌浸润评估的超声视频片段,其中包括5个若发生浸润则表明肿瘤不可切除的部位。对于每个部位,有10个显示癌症浸润的视频片段和10个显示无癌症浸润的视频片段。参考标准为手术发现并经组织学证实或化疗反应。为进行统计分析,将19个部位分为四个解剖区域:盆腔、中腹部、上腹部和淋巴结。视频片段由包括资深妇科医生(主要是自我训练的专家级超声检查人员,几乎每天都进行卵巢癌扩散的术前超声评估)和在妇科肿瘤中心接受过至少6个月卵巢癌扩散术前超声评估监督培训的妇科医生组成的评分者进行评估。根据每年的个人病例量以及他们进行卵巢癌扩散超声评估的年限,评分者被分为经验丰富或经验较少两类。评分者知晓每个部位会有10个有癌症浸润和10个无癌症浸润的视频片段。每位评分者独立将每个视频片段分类为显示或未显示癌症浸润,并对图像质量(从0到10评分)和他们的诊断信心(从0到10评分)进行评级。使用具有随机效应的广义线性混合模型来估计哪些因素(包括经验水平、图像质量、诊断信心和解剖区域)会影响癌症浸润正确分类的可能性。我们评估了正确分类的视频片段的观察百分比、基于广义线性混合模型正确分类的视频片段的预期百分比以及检查人员之间在将解剖部位分类为是否被癌症浸润方面的一致性(可靠性)。
25名评分者参与了研究,其中13名经验丰富,12名经验较少。根据评分者和解剖部位的不同,癌症浸润正确分类的观察百分比范围为70%至100%,25名评分者正确分类中位数百分比范围为90%至100%。所有380个视频片段正确分类的概率范围为0.956至0.975,且不受评分者超声经验水平的影响。正确分类的可能性随着图像质量和诊断信心的提高而增加,并受解剖区域影响。盆腔部位最高,中腹部其次,淋巴结第三,上腹部部位最低。所有25名评分者关于癌症浸润存在与否的检查人员间一致性根据解剖部位不同,从“实质性”(Fleiss卡方值,0.68(95%CI,0.66 - 0.71))到“非常好”(Fleiss卡方值,0.99(95%CI,0.97 - 1.00))不等。上腹部部位最低(Fleiss卡方值,0.68(95%CI,0.66 - 0.71)至0.97(95%CI,0.94 - 0.99)),盆腔部位最高(Fleiss卡方值,0.94(95%CI,0.92 - 0.97)至0.99(95%CI,0.97 - 1.00))。
具有不同超声经验水平的超声检查人员可以根据经验丰富的超声检查人员获取的视频记录,正确地将预定义解剖部位分类为是否被卵巢癌浸润,且检查人员间一致性较强。盆腔部位正确分类的可能性以及检查人员间一致性最高,上腹部部位最低。然而,由于研究设计的原因,我们关于诊断准确性和检查人员间一致性的结果可能过于乐观。© 2025作者。《妇产科超声》由John Wiley & Sons Ltd代表国际妇产科超声学会出版。