Yelverton Valerie, Ostermann Jan, Yarrington Michael E, Lokhnygina Yuliya V, Weinhold Andrew K, Thielman Nathan M
Division of Infectious Diseases, Department of Medicine, Duke University School of Medicine, Durham, NC, USA.
Department of Health Services Policy and Management, University of South Carolina, Arnold School of Public Health, Columbia, SC, USA.
Mhealth. 2025 Mar 21;11:18. doi: 10.21037/mhealth-24-69. eCollection 2025.
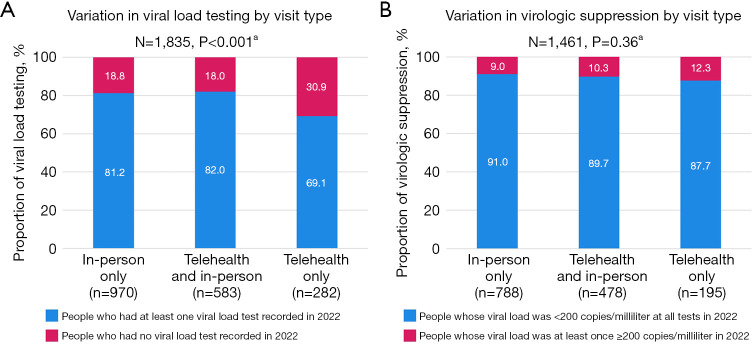
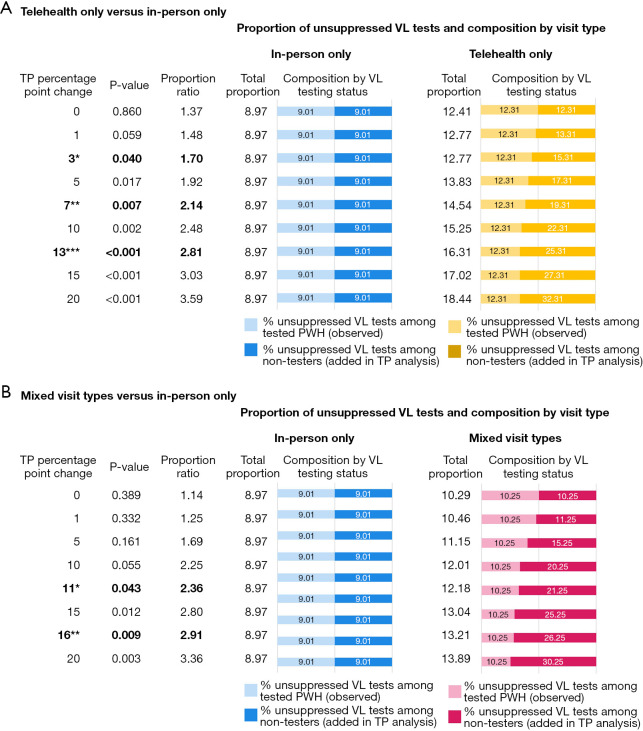
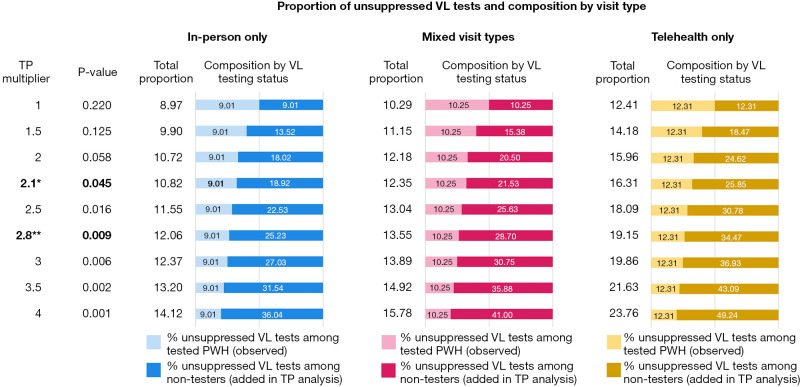
While telehealth was widely used to provide human immunodeficiency virus (HIV) care during the coronavirus disease 2019 (COVID-19) pandemic, research evaluating viral suppression by visit type is conflicting. This study assessed variation in viral load (VL) testing and outcomes by visit type for routine HIV care visits among people living with HIV (PWH) at a large academic health center in central North Carolina (NC). Electronic health records (EHRs) data from the Duke University Infectious Disease (ID) Clinic in NC were extracted in aggregated form. Pearson's Chi-square (χ) tests were used to examine variation in VL testing and virologic suppression (VS) in 2022 by visit type patterns in the first year of the pandemic. Tipping point (TP) sensitivity analyses were conducted. EHR data from 1,835 PWH were included. Between March 16, 2020 and March 15, 2021, 53% of PWH received in-person HIV care only, 32% received a combination of telehealth and in-person care, and 15% received telehealth care only. About 20% of PWH did not have any VL test recorded in 2022. Among PWH with a VL test, 90% were virologically suppressed at all tests in 2022. Visit type was significantly associated with VL testing (P<0.001). The proportion of people who had no VL test in 2022 was larger among telehealth only users (31%) as compared to in-person only or PWH who received a combination (19% and 18%, respectively). VS in 2022 did not differ by visit type pattern in the first year of the pandemic (P=0.36) among PWH with a VL test in 2022. TP analyses identified that the proportion of unsuppressed VL tests among PWH without any VL test in 2022 would need to be multiplied by 2.1 to result in a statistically significant difference in VS by visit type (P=0.045). Our findings indicate that VL outcomes among telehealth users who had VL testing results documented in EHR at least one year later did not differ from in-person HIV care users. However, VL testing uptake was lower among telehealth only users suggesting the need for strategies such as remote VL testing to ensure regular VL testing among PWH who use telehealth HIV care.
在2019冠状病毒病(COVID-19)大流行期间,远程医疗被广泛用于提供人类免疫缺陷病毒(HIV)护理,但评估不同就诊类型对病毒抑制效果的研究结果存在冲突。本研究评估了北卡罗来纳州中部一家大型学术健康中心的HIV感染者(PWH)在进行常规HIV护理就诊时,不同就诊类型的病毒载量(VL)检测及结果的差异。从北卡罗来纳州杜克大学传染病(ID)诊所提取了汇总形式的电子健康记录(EHR)数据。采用Pearson卡方(χ²)检验,以研究2022年大流行第一年不同就诊类型模式下的VL检测及病毒学抑制(VS)情况。进行了临界点(TP)敏感性分析。纳入了1835名PWH的EHR数据。在2020年3月16日至2021年3月15日期间,53%的PWH仅接受面对面HIV护理,32%接受远程医疗与面对面护理相结合的方式,15%仅接受远程医疗护理。2022年约20%的PWH没有任何VL检测记录。在有VL检测记录的PWH中,90%在2022年的所有检测中病毒学得到抑制。就诊类型与VL检测显著相关(P<0.001)。仅使用远程医疗的用户中,2022年未进行VL检测的比例(31%)高于仅接受面对面护理或接受两种护理方式结合的PWH(分别为19%和18%)。在2022年有VL检测记录的PWH中,大流行第一年不同就诊类型模式下的VS情况无差异(P=0.36)。TP分析表明,2022年没有任何VL检测记录的PWH中未被抑制的VL检测比例需乘以2.1,才能使不同就诊类型的VS产生统计学显著差异(P=0.045)。我们的研究结果表明,至少一年后在EHR中有VL检测结果记录的远程医疗用户的VL结果与接受面对面HIV护理的用户无差异。然而,仅使用远程医疗的用户中VL检测的接受度较低,这表明需要采取如远程VL检测等策略,以确保使用远程医疗HIV护理的PWH能定期进行VL检测。