Shi Zhongyong, Ma Xin, Tang Tianyi, Wang Meijuan, Zheng Hailin, Chen Yupeng, Hu Jingxiao, Mueller Ariel, Houle Timothy T, Marcantonio Edward R, Xie Zhongcong, Shen Yuan
Shanghai Mental Health Center, Shanghai Jiao Tong University School of Medicine, Shanghai, China.
Anesthesia and Brain Research Institute, Tongji University School of Medicine, Shanghai, China.
Gen Psychiatr. 2025 Apr 1;38(2):e101740. doi: 10.1136/gpsych-2024-101740. eCollection 2025.
Postoperative delirium is one of the most common complications in the older surgical population, but its pathogenesis and biomarkers are largely undetermined. Retinal layer thickness has been demonstrated to be associated with cognitive function in mild cognitive impairment and patients with Alzheimer's disease. However, relatively little is known about possible retinal layer thickness among patients with postoperative delirium.
We aimed to investigate the relationship between retinal layer thickness and postoperative delirium in this cross-sectional study.
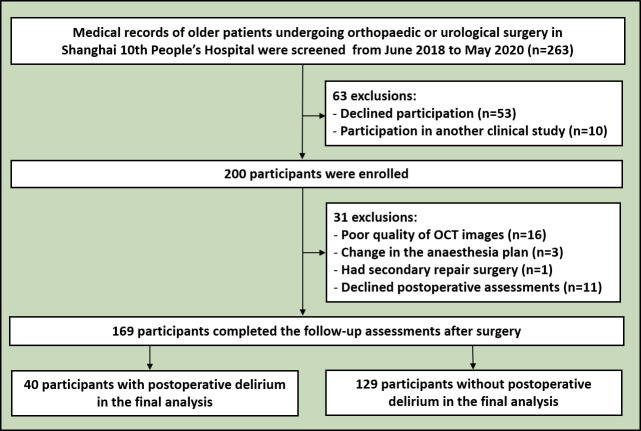
The participants (≥65 years old) having elective surgery under general anaesthesia were screened via medical records from Shanghai 10th People's Hospital. Preoperative macular thickness and peripapillary retinal nerve fibre layer (RNFL) thickness were measured using optical coherence tomography (OCT). The Confusion Assessment Method (CAM) algorithm and CAM-Severity (CAM-S) were used to assess the incidence and severity of postoperative delirium on the first, second and third days after surgery.
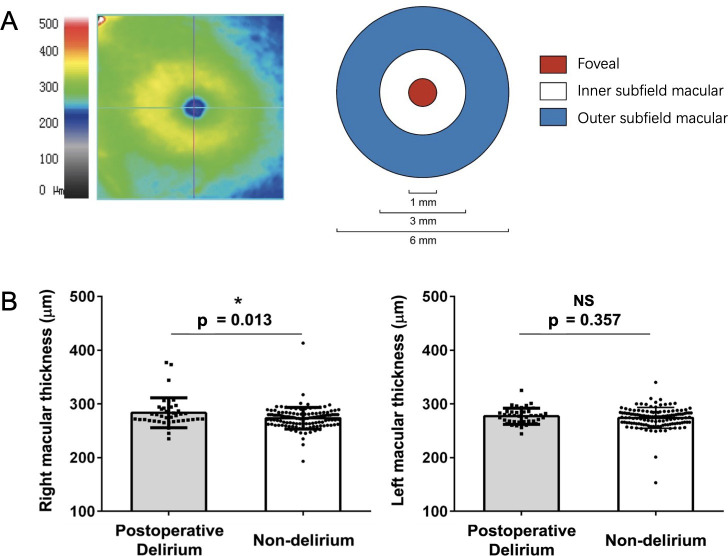
Among 169 participants (mean (standard deviation (SD) 71.15 (4.36) years), 40 (24%) developed postoperative delirium. Notably, individuals who developed postoperative delirium exhibited thicker preoperative macular thickness in the right eye compared with those who did not (mean (SD) 283.35 (27.97) µm vs 273.84 (20.14) µm, p=0.013). Furthermore, the thicker preoperative macular thickness of the right eye was associated with a higher incidence of postoperative delirium (adjusted odds ratio 1.593, 95% confidence interval (CI) 1.093 to 2.322, p=0.015) and greater severity (adjusted mean difference ()=0.256, 95% CI 0.037 to 0.476, p=0.022) after adjustment for age, sex and Mini-Mental State Examination (MMSE) scores. However, such a difference or association did not appear in the left macular or bilateral peripapillary RNFL thicknesses.
Current findings demonstrated that preoperative macular thickness might serve as a potential non-invasive marker for the vulnerability of developing postoperative delirium in older surgical patients. Further large-scale validation studies should be performed to confirm these results.
术后谵妄是老年外科患者中最常见的并发症之一,但其发病机制和生物标志物在很大程度上仍未明确。视网膜层厚度已被证明与轻度认知障碍和阿尔茨海默病患者的认知功能有关。然而,关于术后谵妄患者的视网膜层厚度情况,人们了解相对较少。
在这项横断面研究中,我们旨在探讨视网膜层厚度与术后谵妄之间的关系。
通过上海第十人民医院的病历筛选接受全身麻醉下择期手术的参与者(≥65岁)。使用光学相干断层扫描(OCT)测量术前黄斑厚度和视盘周围视网膜神经纤维层(RNFL)厚度。采用意识模糊评估法(CAM)算法和CAM严重程度(CAM-S)评估术后第1、2和3天谵妄的发生率和严重程度。
在169名参与者(平均(标准差(SD))71.15(4.36)岁)中,40名(24%)发生了术后谵妄。值得注意的是,发生术后谵妄的个体右眼术前黄斑厚度比未发生者厚(平均(SD)283.35(27.97)µm对273.84(20.14)µm,p=0.013)。此外,调整年龄、性别和简易精神状态检查表(MMSE)评分后,右眼术前黄斑厚度越厚,术后谵妄的发生率越高(调整优势比1.593,95%置信区间(CI)1.093至2.322,p=0.015),严重程度越高(调整平均差()=0.256,95%CI 0.037至0.476,p=0.022)。然而,这种差异或关联在左眼黄斑或双侧视盘周围RNFL厚度中未出现。
目前的研究结果表明,术前黄斑厚度可能是老年外科患者发生术后谵妄易感性的潜在非侵入性标志物。应进行进一步的大规模验证研究以证实这些结果。