Saito Yuichi, Shiko Yuki, Tateishi Kazuya, Toda Koichi, Matsumiya Goro, Kobayashi Yoshio
Department of Cardiovascular Medicine Chiba University Graduate School of Medicine Chiba Japan.
Biostatistics Section, Clinical Research Center Chiba University Hospital Chiba Japan.
J Am Heart Assoc. 2025 May 6;14(9):e040487. doi: 10.1161/JAHA.124.040487. Epub 2025 Apr 25.
In patients with cardiogenic shock (CS), a percutaneous microaxial ventricular assist device (Impella, Abiomed, Danvers, MA) is a choice for temporary mechanical circulatory support. Given the high morbidity and mortality in this patient population, early risk stratification is relevant when making treatment decisions.
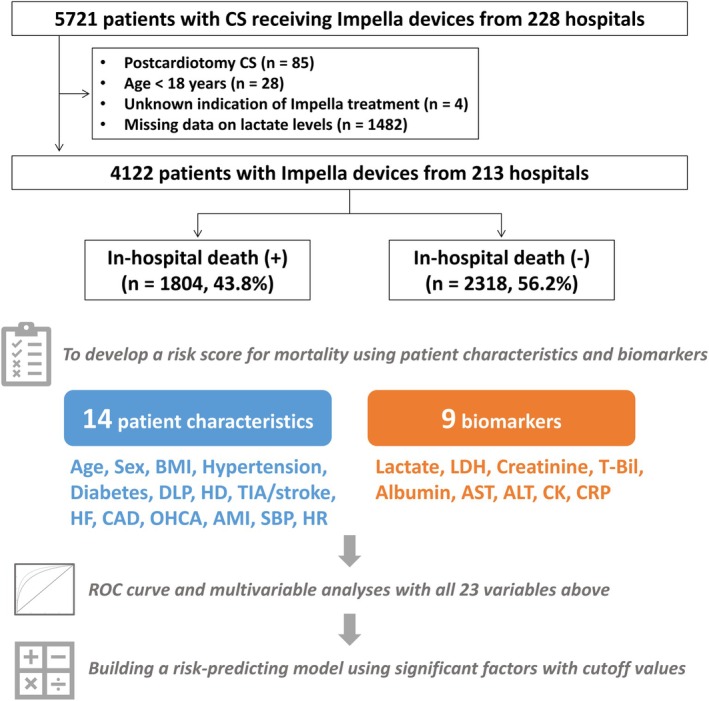
Using nationwide registry data between February 2020 and December 2022 in Japan, we included a total of 4122 patients with cardiogenic shock treated with the Impella devices. Using logistic regression analysis, we incorporated patient characteristics and biomarkers to develop a risk-stratifying model for in-hospital mortality. The model was also tested if applicable to composite outcomes of in-hospital death and major complications.
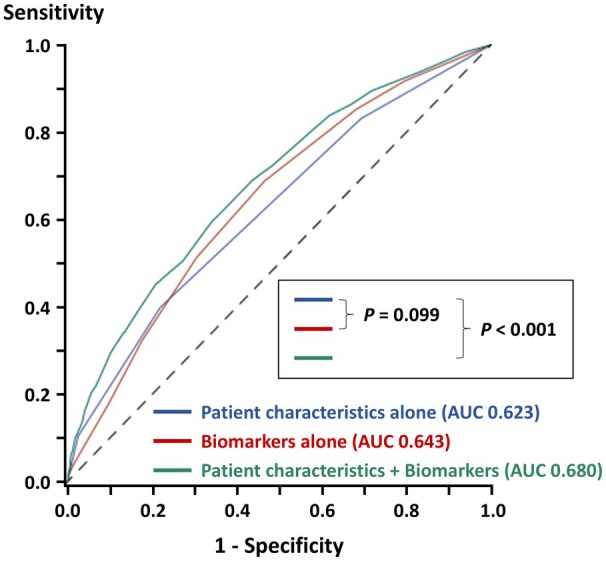
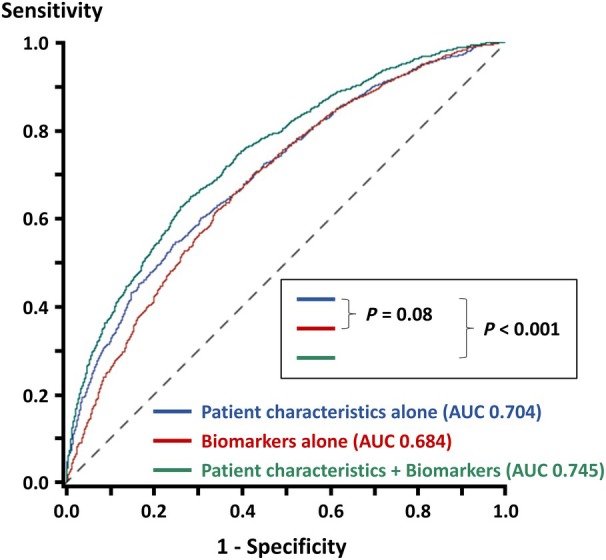
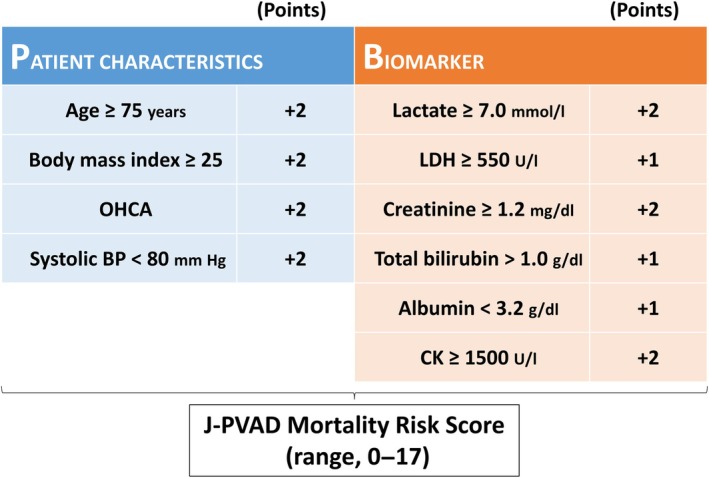
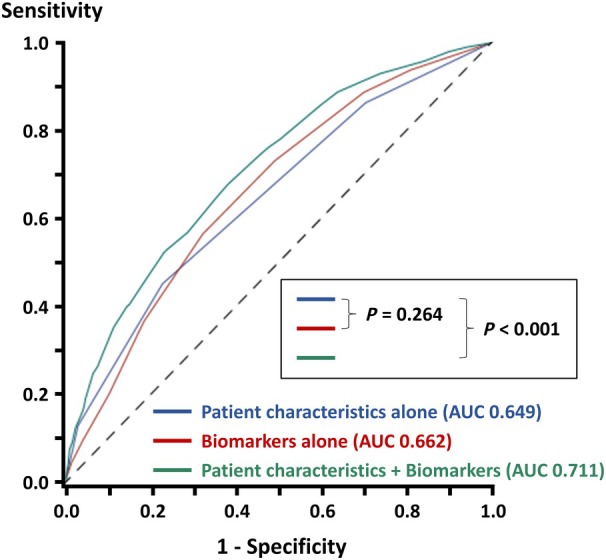
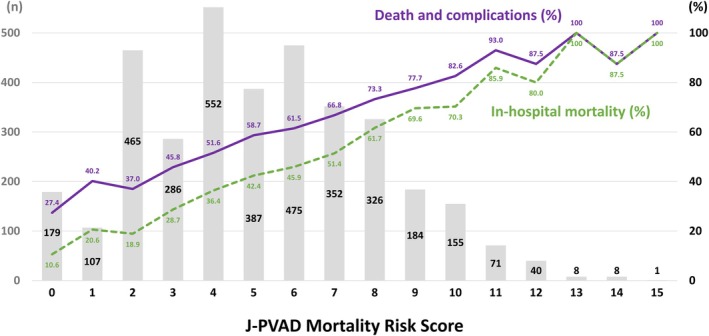
Of the 4122 patients with cardiogenic shock, the Impella was indicated for acute myocardial infarction in 2575 (62.5%). Multivariable analysis identified 4 patient characteristics (age, body mass index, out-of-hospital cardiac arrest, and blood pressure) and 6 biomarkers (lactate, lactate dehydrogenase, creatinine, total bilirubin, albumin, and creatinine kinase) with cutoff values as factors significantly associated with in-hospital mortality. We developed a risk-stratifying model using the 10 variables, which was predictive of in-hospital death (area under the curve, 0.711; <0.001). Adding biomarkers to patient characteristics significantly improved the diagnostic accuracy (area under the curve, from 0.649 to 0.711; <0.001). This risk score was also predictive of death and major complications (area under the curve, 0.680; <0.001).
In patients with cardiogenic shock treated with the Impella devices, our risk-stratifying system, consisting of 4 patient characteristics and 6 biomarkers, strongly correlated with in-hospital mortality, potentially facilitating clinical decision-making.
在心源 性休克(CS)患者中,经皮微轴心室辅助装置(Impella,Abiomed,丹弗斯,马萨诸塞州)是临时机械循环支持的一种选择。鉴于该患者群体的高发病率和死亡率,在做出治疗决策时进行早期风险分层具有重要意义。
利用日本2020年2月至2022年12月期间的全国登记数据,我们纳入了总共4122例接受Impella装置治疗的心源性休克患者。使用逻辑回归分析,我们纳入患者特征和生物标志物来建立院内死亡风险分层模型。还测试了该模型是否适用于院内死亡和主要并发症的复合结局。
在4122例心源性休克患者中,Impella用于急性心肌梗死的有2575例(62.5%)。多变量分析确定了4个患者特征(年龄、体重指数、院外心脏骤停和血压)和6种生物标志物(乳酸、乳酸脱氢酶、肌酐、总胆红素、白蛋白和肌酸激酶)及其临界值为与院内死亡显著相关的因素。我们使用这10个变量建立了一个风险分层模型,该模型可预测院内死亡(曲线下面积,0.711;P<0.001)。将生物标志物添加到患者特征中可显著提高诊断准确性(曲线下面积,从0.649提高到0.711;P<0.001)。该风险评分也可预测死亡和主要并发症(曲线下面积,0.680;P<0.001)。
在接受Impella装置治疗的心源性休克患者中,我们由4个患者特征和6种生物标志物组成的风险分层系统与院内死亡率密切相关,可能有助于临床决策。