d'Elbée Marc, Mafirakureva Nyashadzaishe, Chabala Chishala, Huyen Ton Nu Nguyet Minh, Harker Martin, Roucher Clémentine, Businge Gerald, Shankalala Perfect, Nduna Bwendo, Mulenga Veronica, Bonnet Maryline, Wobudeya Eric, Marcy Olivier, Dodd Peter J
University of Bordeaux, National Institute for Health and Medical Research (Inserm) UMR 1219, Research Institute for Sustainable Development (IRD) EMR 271, Bordeaux, France.
Sheffield Centre for Health & Related Research (SCHARR), University of Sheffield, Sheffield, United Kingdom.
EClinicalMedicine. 2025 Apr 19;83:103206. doi: 10.1016/j.eclinm.2025.103206. eCollection 2025 May.
Children with severe acute malnutrition (SAM) are an important risk group for underdiagnosis and death from tuberculosis. In 2022, the World Health Organization (WHO) recommended use of treatment decision algorithms (TDAs) for tuberculosis diagnosis in children. There is currently no cost-effectiveness evidence for TDA-based approaches compared to routine practice.
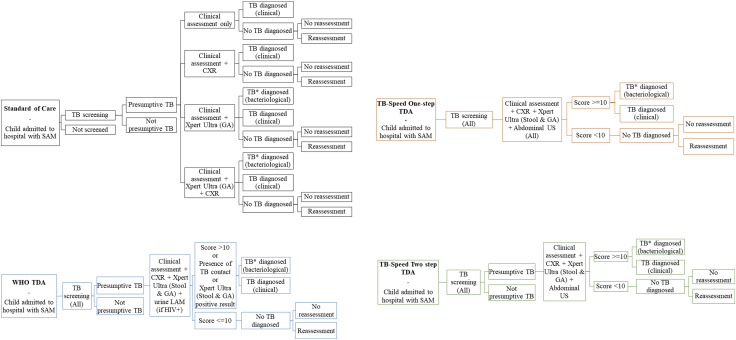
The TB-Speed SAM study developed i) a one-step TDA including Xpert, clinical, radiological and echography features, and ii) a two-step TDA, which also included a screening phase, for children under 5 years hospitalised with SAM at three tertiary hospitals in Uganda and Zambia from 4th November 2019 to 20th June 2022. This study is registered with ClinicalTrials.gov, NCT04240990. We assessed the diagnostic accuracy and cost-effectiveness of deploying TB-Speed and WHO TDA-based approaches compared to the standard of care (SOC). Estimated outcomes included children started on tuberculosis treatment, false positive rates, disability-adjusted life years (DALYs) and incremental cost-effectiveness ratios (ICERs).
Per 100 children hospitalised with SAM, averaging 19 children with tuberculosis, the one-step TDA initiated 17 true positive children (95% uncertainty intervals [UI]: 12-23) on tuberculosis treatment, the two-step TDA 15 (95%UI: 10-22), the WHO TDA 14 (95%UI: 9-19), and SOC 4 (95%UI: 2-9). The WHO TDA generated the most false positives (35, 95%UI: 24-46), followed by the one-step TDA (18, 95%UI: 6-29), the two-step TDA (14, 95%UI: 1-25), and SOC (11, 95%UI: 3-17). All TDA-based approaches had ICERs below plausible country cost-effectiveness thresholds compared to SOC (one-step: $44-51/DALY averted, two-step: $34-39/DALY averted, WHO: $40-46/DALY averted).
Our findings show that these TDA-based approaches are highly cost-effective for the vulnerable group of children hospitalised with SAM, compared to current practice.
Unitaid Grant number: 2017-15-UBx-TB-SPEED.
患有重度急性营养不良(SAM)的儿童是结核病漏诊和死亡的重要风险群体。2022年,世界卫生组织(WHO)建议使用治疗决策算法(TDA)对儿童结核病进行诊断。与常规做法相比,目前尚无基于TDA方法的成本效益证据。
“结核病-快速诊断重度急性营养不良”(TB-Speed SAM)研究针对2019年11月4日至2022年6月20日期间在乌干达和赞比亚三家三级医院住院治疗的5岁以下重度急性营养不良儿童,开发了:i)一种包括Xpert、临床、放射学和超声特征的一步式TDA;ii)一种两步式TDA,其中还包括一个筛查阶段。本研究已在ClinicalTrials.gov注册,注册号为NCT04240990。我们评估了与标准治疗(SOC)相比,采用基于TB-Speed和WHO TDA方法的诊断准确性和成本效益。估计结果包括开始接受结核病治疗的儿童、假阳性率、伤残调整生命年(DALY)和增量成本效益比(ICER)。
每100名因重度急性营养不良住院的儿童中,平均有19名患有结核病,一步式TDA使17名真正阳性儿童(95%不确定区间[UI]:12-23)开始接受结核病治疗,两步式TDA使15名(95%UI:10-22),WHO TDA使14名(95%UI:9-19),标准治疗使4名(95%UI:2-9)。WHO TDA产生的假阳性最多(35例,95%UI:24-46),其次是一步式TDA(18例,95%UI:6-29),两步式TDA(14例,95%UI:1-25),标准治疗(11例,95%UI:3-17)。与标准治疗相比,所有基于TDA的方法的ICER均低于合理的国家成本效益阈值(一步式:每避免一个DALY节省44-51美元,两步式:每避免一个DALY节省34-39美元,WHO:每避免一个DALY节省40-46美元)。
我们的研究结果表明,与目前的做法相比,这些基于TDA的方法对于因重度急性营养不良住院的儿童这一弱势群体具有很高的成本效益。
联合国国际药品采购机制(Unitaid)资助编号:2017-15-UBx-TB-SPEED。