Gao Huayuan, Wu Junmei, Chen Youwen, Wang Chengyu, Yao Minmin, Yang Yan, Miao Changhong, Liang Chao
Department of Anesthesiology, Zhongshan Hospital (Xiamen), Fudan University, Xiamen, Fujian, People's Republic of China.
Department of Anesthesiology, Zhongshan Hospital, Fudan University, Shanghai, People's Republic of China.
Drug Des Devel Ther. 2025 Apr 24;19:3129-3138. doi: 10.2147/DDDT.S508736. eCollection 2025.
This study aimed to determine the 95% effective concentration (EC) of propofol via target-controlled infusion (TCI) for endotracheal intubation at three different doses of dexmedetomidine.
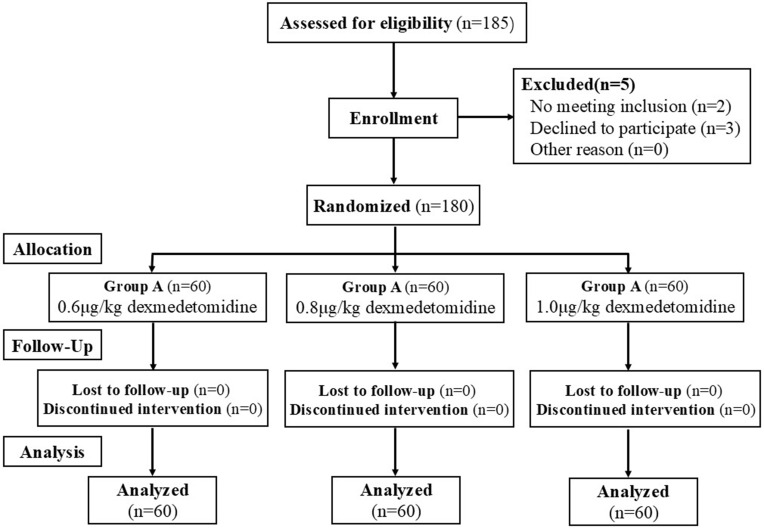
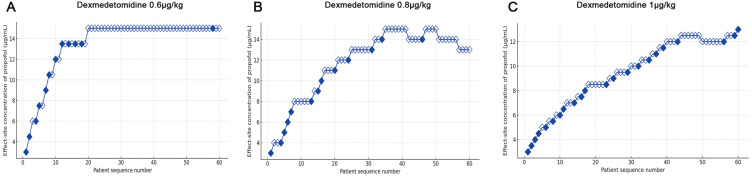
One hundred and eighty patients aged 18-60 and classified as American Society of Anesthesiologists (ASA) class I-II were enrolled to undergo general anesthesia. Patients were randomly assigned to one of the three groups (A, B, or C), receiving three different doses of dexmedetomidine (0.6, 0.8, or 1 μg/kg) infused over 10 min. Anesthesia was then induced with propofol TCI, followed by rocuronium. The biased coin design method was used to calculate the EC of propofol for successful intubation. The primary outcome endpoint was the EC of propofol for successful endotracheal intubation at each dexmedetomidine dose.
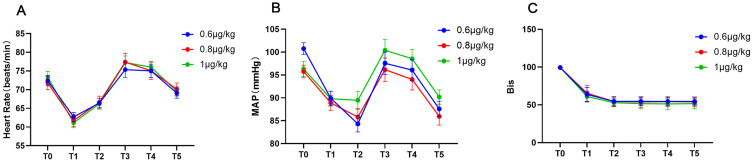
Sixty patients in each group completed the trial. The time from propofol administration to intubation in group C (132.5 ± 10.7 s) was significantly shorter compared to group A (140.2 ± 14.4 s, <0.0001) and group B (142.6 ± 13.2 s, =0.0037). Both the EC and the average total dose of propofol in group B [14.6 (10.8, 14.8) μg/mL and 3.6 ± 1.1 mg/kg] and C [12.7 (11.5, 12.8) μg/mL and 2.8 ± 1.0 mg/kg] were lower than those in group A [14.9 (4.5, 15.0) μg/mL and 3.8 ± 0.9 mg/kg] (<0.001). The incidence of hypotension and bradycardia during induction was low in each group.
The EC of propofol for endotracheal intubation across three different background doses of dexmedetomidine was determined. We suggest administering 1.0 μg/kg dexmedetomidine and then the EC of propofol for successful endotracheal intubation was 12.7 μg/mL.
Chinese Clinical Trial Registry; Registration number: ChiCTR2400089952, URL:https://www.chictr.org.cn/showproj.html?proj=221236.
本研究旨在确定在三种不同剂量右美托咪定情况下,通过靶控输注(TCI)丙泊酚用于气管插管的95%有效浓度(EC)。
纳入18 - 60岁、美国麻醉医师协会(ASA)分级为I - II级的180例患者行全身麻醉。患者随机分为三组(A、B或C组),接受三种不同剂量的右美托咪定(0.6、0.8或1μg/kg),于10分钟内输注完毕。然后用丙泊酚TCI诱导麻醉,随后给予罗库溴铵。采用偏倚硬币设计法计算丙泊酚用于成功插管的EC。主要结局终点是各右美托咪定剂量下丙泊酚用于成功气管插管的EC。
每组60例患者完成试验。C组从给予丙泊酚到插管的时间(132.5±10.7秒)显著短于A组(140.2±14.4秒,<0.0001)和B组(142.6±13.2秒,=0.0037)。B组[14.6(10.8,14.8)μg/mL和3.6±1.1mg/kg]和C组[12.7(11.5,12.8)μg/mL和2.8±1.0mg/kg]丙泊酚的EC及平均总剂量均低于A组[14.9(4.5,15.0)μg/mL和3.8±0.9mg/kg](<0.001)。每组诱导期间低血压和心动过缓的发生率较低。
确定了三种不同背景剂量右美托咪定情况下丙泊酚用于气管插管的EC。我们建议给予1.0μg/kg右美托咪定,然后丙泊酚用于成功气管插管的EC为12.7μg/mL。
中国临床试验注册中心;注册号:ChiCTR2400089952,网址:https://www.chictr.org.cn/showproj.html?proj=221236 。