Igarashi Ataru, Tachimori Hisateru, Maruyama-Sakurai Keiko, Segawa Yasumasa, Takagi Hiroyuki, Akiyama Hiroki, Imai Naohiko, Kohsaka Shun, Miyata Hiroaki
Department of Health Economics and Outcomes Research, Graduate School of Pharmaceutical Sciences, The University of Tokyo, 7-3-1 Hongo, Bunkyo-ku, Tokyo, 113-0033, Japan.
Graduate School of Data Sciences, Yokohama City University School of Medicine, Kanagawa, Japan.
Adv Ther. 2025 Jun;42(6):2888-2905. doi: 10.1007/s12325-025-03157-z. Epub 2025 Apr 29.
Cardiovascular, renal, and metabolic diseases, collectively known as cardio-renal-metabolic (CRM) disease, interact and exacerbate each other, creating serious clinical and economic burdens. Sodium-glucose cotransporter 2 inhibitors (SGLT2i) are important therapeutic agents in managing CRM disease. Despite proven clinical benefits, the economic benefits of SGLT2i in the management of CRM diseases remain unclear.
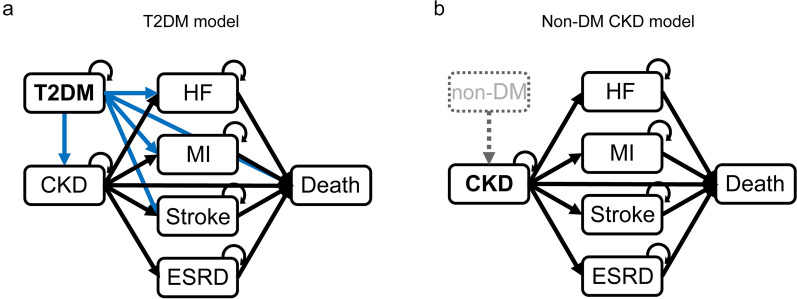
We developed Markov models representing the natural progression of disease for two populations: a type 2 diabetes mellitus (T2DM) population and non-diabetic chronic kidney disease (non-DM CKD) population. These models incorporated key complications, including heart failure, myocardial infarction, stroke, CKD (for the T2DM population), and end-stage renal disease. A systematic literature search was conducted to determine input parameters. For each model, we estimated the 10-year medical costs, quality-adjusted life years (QALY), and incremental cost-effectiveness ratio (ICER) for SGLT2i treatment compared with conventional treatment. A probabilistic sensitivity analysis (PSA) and scenario analyses with conservative assumptions were performed.
In the base-case analysis, SGLT2i treatment was estimated to increase QALY by 0.177 (7.090 vs 6.913 QALY; T2DM population) and 0.457 (6.980 vs 6.523 QALY; non-DM CKD population), and increase total medical costs by Japanese yen (JPY) 99,060 (JPY 762,524 vs 663,463; T2DM population) and JPY 229,810 (JPY 3,378,873 vs 3,149,063; non-DM CKD population), compared with conventional treatment. The ICER was JPY 559,175/QALY in the T2DM population and JPY 503,123/QALY in the non-DM CKD population. The PSA revealed that the probability of ICER being below the threshold value of JPY 5,000,000/QALY was 100% in the T2DM population and 98.7% in the non-DM CKD population, and the ICERs were below this threshold in all scenario analyses.
SGLT2i treatment was demonstrated to be cost-effective in both the T2DM population and the non-DM CKD population, suggesting the potential of SGLT2i to offer significant clinical and economic benefits in the comprehensive management of CRM diseases.
心血管疾病、肾脏疾病和代谢性疾病统称为心肾代谢(CRM)疾病,它们相互作用并相互加剧,造成严重的临床和经济负担。钠-葡萄糖协同转运蛋白2抑制剂(SGLT2i)是管理CRM疾病的重要治疗药物。尽管已证实其具有临床益处,但SGLT2i在CRM疾病管理中的经济效益仍不明确。
我们开发了马尔可夫模型来表示两种人群的疾病自然进展:2型糖尿病(T2DM)人群和非糖尿病慢性肾脏病(非DM CKD)人群。这些模型纳入了关键并发症,包括心力衰竭、心肌梗死、中风、CKD(针对T2DM人群)和终末期肾病。进行了系统的文献检索以确定输入参数。对于每个模型,我们估计了与传统治疗相比,SGLT2i治疗的10年医疗成本、质量调整生命年(QALY)和增量成本效益比(ICER)。进行了概率敏感性分析(PSA)和采用保守假设的情景分析。
在基础案例分析中,估计SGLT2i治疗与传统治疗相比,可使T2DM人群的QALY增加0.177(分别为7.090和6.913 QALY),使非DM CKD人群的QALY增加0.457(分别为6.980和6.523 QALY),并使T2DM人群的总医疗成本增加99,060日元(分别为762,524日元和663,463日元),使非DM CKD人群的总医疗成本增加229,810日元(分别为3,378,873日元和3,149,063日元)。T2DM人群的ICER为559,175日元/QALY,非DM CKD人群的ICER为503,123日元/QALY。PSA显示,T2DM人群中ICER低于5,000,000日元/QALY阈值的概率为100%,非DM CKD人群中为98.7%,并且在所有情景分析中ICER均低于该阈值。
SGLT2i治疗在T2DM人群和非DM CKD人群中均被证明具有成本效益,这表明SGLT2i在CRM疾病的综合管理中具有提供显著临床和经济效益的潜力。