Nagendra Danavath, Chaudhuri Souvik, Gupta Nitin, Shanbhag Vishal, Eshwara Vandana K, Rao Shwethapriya, Varma Muralidhar, Srinivas Thejesh, Todur Pratibha, Priya P S, Bhat Vinutha R
Department of Critical Care, Kasturba Medical College, Manipal, Manipal Academy of Higher Education, Manipal, Karnataka, India.
Department of Infectious Diseases, Kasturba Medical College, Manipal, Manipal Academy of Higher Education, Manipal, Karnataka, India.
Indian J Crit Care Med. 2025 Apr;29(4):370-393. doi: 10.5005/jp-journals-10071-24957.
Hypervirulent (HvKp) is a virulent strain associated with invasive infections. While initially community-acquired, hospital-acquired HvKp (HA-HvKp) and carbapenem-resistant HvKp (CR-HvKp) are increasingly reported. This meta-analysis evaluates the prevalence, risk factors, and clinical outcomes associated with HvKp, including CR-HvKp and HA-HvKp, among Kp infections.
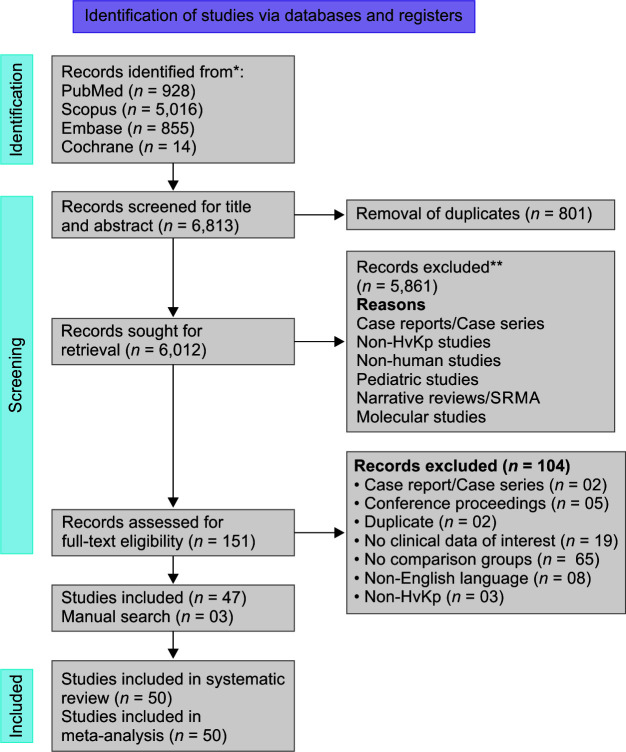
A systematic search of PubMed, Scopus, Embase, and Cochrane Library was conducted until December 2024. Observational studies comparing HvKp vs classical Kp (cKp), CR-HvKp vs carbapenem-sensitive HvKp (CS-HvKp), and HA-HvKp vs community-acquired HvKp (CA-HvKp) were included. Quality was assessed using the Joanna Briggs Critical Appraisal Tool, and pooled prevalence and odds ratios (ORs) with 95% confidence intervals (CIs) were calculated.
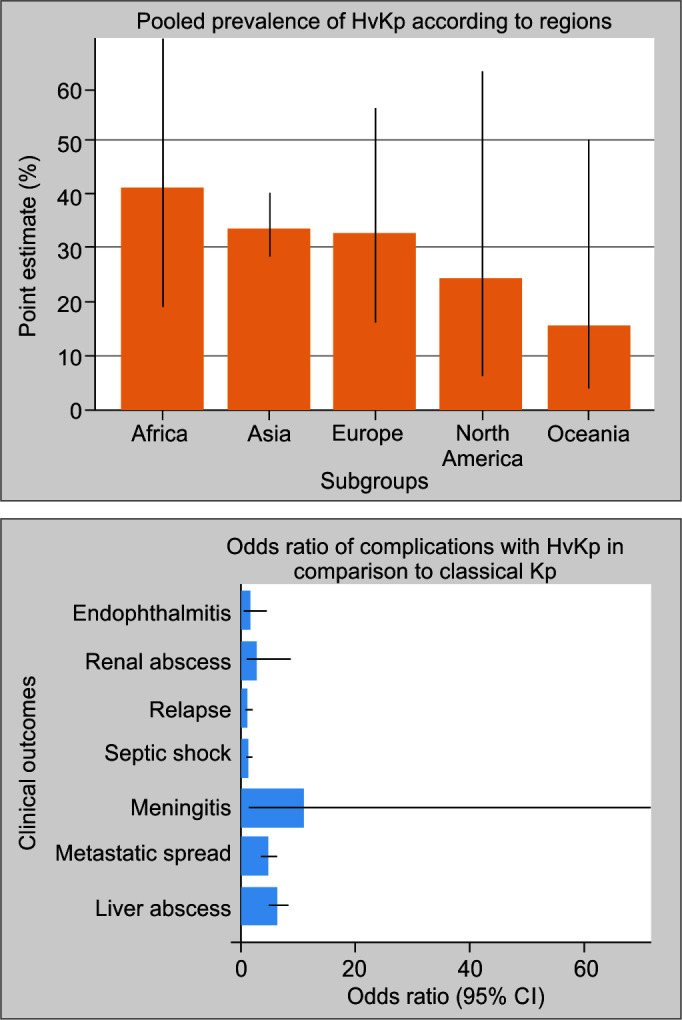
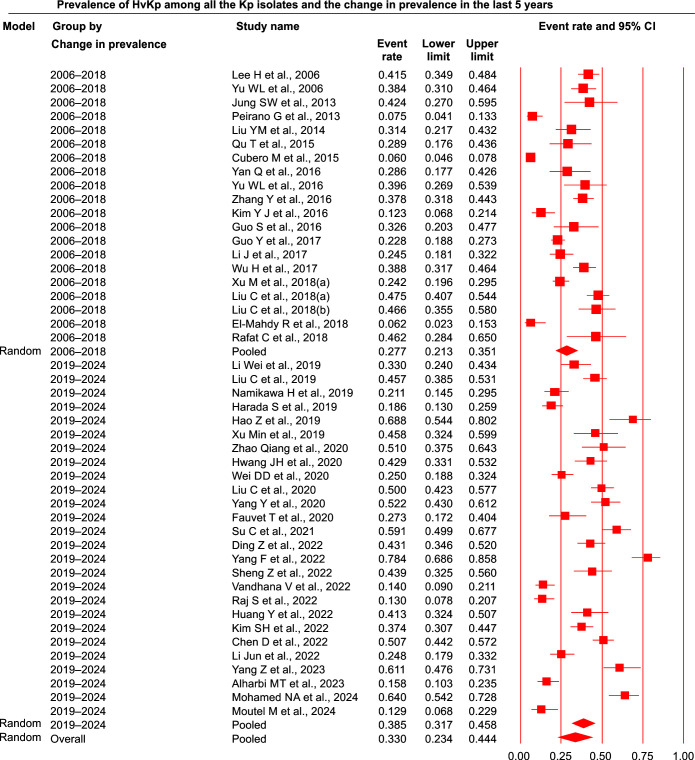
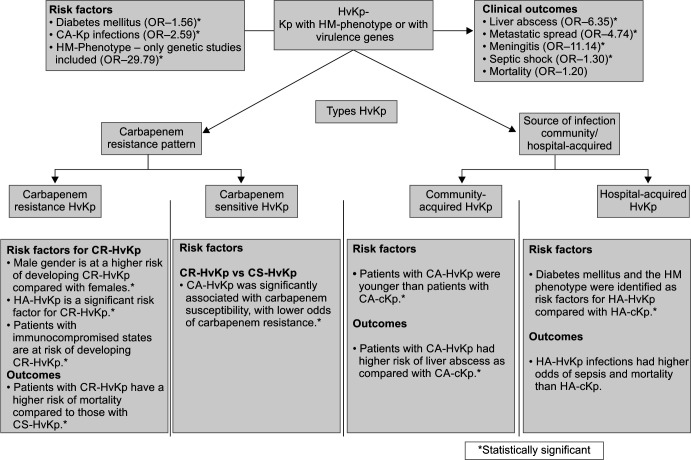
Fifty studies with 6,663 participants were included. The HvKp prevalence was 33.0%, with most studies from Asia, predominantly China. Temporal analysis revealed an increase in HvKp prevalence (27.7% in 2006-2018 to 38.5% in 2019-2024). The CR-HvKp prevalence rose from 9.5% to 16.5% (2016-2024). The HA-HvKp prevalence increased from 25.9 to 47.1%. Key risk factors included diabetes mellitus (OR = 1.56), CA-Kp (OR = 2.59), and hypermucoviscous (HM)-phenotype (OR = 29.79). Complications included liver abscess (OR = 6.35), metastatic spread (OR = 4.74), meningitis (OR = 11.14), and septic shock (OR = 1.30). Mortality was higher in HvKp infections but not statistically significant ( = 0.219). HA-HvKp and immunosuppression were significant CR-HvKp risk factors, with CR-HvKp showing higher mortality.
Diabetes mellitus, CA-Kp infections, and HM-phenotype are significant risk factors for HvKp. The rising prevalence of CR-HvKp and HA-HvKp highlights the need for early detection, infection control, and targeted treatment strategies.
Nagendra D, Chaudhuri S, Gupta N, Shanbhag V, Eshwara VK, Rao S, . Prevalence, Risk Factors, and Clinical Outcomes of Hypervirulent Strains among Infections: A Systematic Review and Meta-analysis. Indian J Crit Care Med 2025;29(4):370-393.
高毒力肺炎克雷伯菌(HvKp)是一种与侵袭性感染相关的毒力菌株。虽然最初是社区获得性的,但医院获得性HvKp(HA-HvKp)和碳青霉烯耐药HvKp(CR-HvKp)的报道越来越多。本荟萃分析评估了与HvKp相关的患病率、危险因素和临床结局,包括CR-HvKp和HA-HvKp在肺炎克雷伯菌感染中的情况。
截至2024年12月,对PubMed、Scopus、Embase和Cochrane图书馆进行了系统检索。纳入了比较HvKp与经典肺炎克雷伯菌(cKp)、CR-HvKp与碳青霉烯敏感HvKp(CS-HvKp)以及HA-HvKp与社区获得性HvKp(CA-HvKp)的观察性研究。使用乔安娜·布里格斯批判性评价工具评估质量,并计算合并患病率和比值比(OR)以及95%置信区间(CI)。
纳入了50项研究,共6663名参与者。HvKp患病率为33.0%,大多数研究来自亚洲,主要是中国。时间分析显示HvKp患病率有所增加(2006 - 2018年为27.7%,2019 - 2024年为38.5%)。CR-HvKp患病率从9.5%上升至16.5%(2016 - 2024年)。HA-HvKp患病率从25.9%增至47.1%。关键危险因素包括糖尿病(OR = 1.56)、社区获得性肺炎克雷伯菌(CA-Kp,OR = 2.59)和高黏液性(HM)表型(OR = 29.79)。并发症包括肝脓肿(OR = 6.35)、转移性扩散(OR = 4.74)、脑膜炎(OR = 11.14)和感染性休克(OR = 1.30)。HvKp感染的死亡率较高,但无统计学显著性(P = 0.219)。HA-HvKp和免疫抑制是CR-HvKp的重要危险因素,CR-HvKp显示出更高的死亡率。
糖尿病、CA-Kp感染和HM表型是HvKp的重要危险因素。CR-HvKp和HA-HvKp患病率的上升凸显了早期检测、感染控制和靶向治疗策略的必要性。
Nagendra D, Chaudhuri S, Gupta N, Shanbhag V, Eshwara VK, Rao S, 。高毒力菌株在肺炎克雷伯菌感染中的患病率、危险因素和临床结局:一项系统评价和荟萃分析。《印度重症监护医学杂志》2025;29(4):370 - 393。