Nketiah-Amponsah Edward, Ahimah-Agyakwah Solomon, Alhassan Robert Kaba, Sunkwa-Mills Gifty, Gómez-Pérez G P, van Andel Judith, Attachey Alex Yao Israel, Opoku-Boateng Yaw Nyarko, Addo-Cobbiah Vivian, Okoe-Boye Bernard, de Wit Tobias Floris Rinke, Antwi Maxwell Akwasi
Department of Economics, University of Ghana, Legon, Accra, Ghana.
Centre for Health Policy and Implementation Research, Institute of Health Research, University of Health and Allied Sciences, Ho, Ghana.
Trop Med Health. 2025 May 6;53(1):65. doi: 10.1186/s41182-025-00743-3.
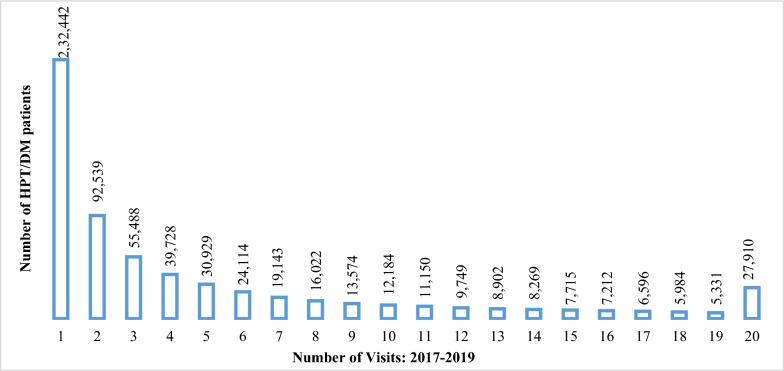
Hypertension (HPT) and diabetes mellitus (DM) are major contributors to morbidity and mortality in Ghana. A key challenge in managing these conditions is non-adherence to follow-up visits, commonly referred to as "lost- to- follow-up" (LTFU). Data from the National Health Insurance Authority (NHIA) between 2017 and 2019 revealed that 37% (232,442/634,981) of patients were LTFU at NHIA-accredited health facilities. This study aimed to investigate the factors driving this high LTFU rate in Ghana.
A total of 480 hypertensive and diabetic patients, randomly selected from the NHIA electronic claims database from facilities in the Greater Accra and Ashanti regions between 2019 and 2020, were interviewed. Participants were divided into two groups: LTFU, which consisted of only one visit (351, 73%), and follow-up (FU), which consisted of more than one visit (129, 27%). The sample included patients diagnosed with hypertension only (308, 64%), diabetes only (45, 9%), and both hypertension and diabetes (127, 26%).
No statistically significant socioeconomic differences were observed between the LTFU and FU groups, except in their adherence to follow-up visits. The likelihood of LTFU was higher among patients without follow-up awareness (OR = 2.5, 95% CI: 1.05-4.83), those who felt stigmatized (OR = 15.51, 95% CI: 1.01-238.90), those who attended facilities where physicians were available only some of the time (OR = 7.37, 95% CI: 1.07-50.61), those attending facilities without the necessary diagnostic equipment, those who described the NHIS coverage for DM diagnostic tests as inadequate, and those receiving traditional or herbal treatments (OR = 16.90, 95% CI: 3.12-91.45). Conversely, patients from the Ashanti Region (OR = 0.58, 95% CI: 0.35-0.96), those educated on diagnostic procedures (OR = 0.28, 95% CI: 0.08-0.98), and those whose treatment was not under control (OR = 0.04, 95% CI: 0.00-0.69) were less likely to be LTFU. Additionally, patients diagnosed more than ten years ago (OR = 0.44, 95% CI: 0.24-0.79) and those who were neutral about establishing support groups were less likely to be LTFU.
The study found that lack of follow-up awareness, stigmatization, and preference for traditional or herbal treatments are key drivers of lost-to-follow-up behavior among hypertension and diabetes patients. Thus, remedial policies should include increasing patient education on the importance of follow-up visits, ensuring the availability of essential medications, diagnostic equipment, and physicians, expanding the NHIA financial coverage, and integrating traditional medicine into standard healthcare to improve treatment adherence and reduce LTFU rates.
高血压(HPT)和糖尿病(DM)是加纳发病和死亡的主要原因。管理这些疾病的一个关键挑战是不遵守随访预约,通常称为“失访”(LTFU)。国家健康保险管理局(NHIA)2017年至2019年的数据显示,在NHIA认可的医疗机构中,37%(232,442/634,981)的患者失访。本研究旨在调查导致加纳如此高失访率的因素。
从2019年至2020年大阿克拉和阿散蒂地区医疗机构的NHIA电子索赔数据库中随机选取480名高血压和糖尿病患者进行访谈。参与者分为两组:失访组,仅就诊一次(351人,73%);随访组,就诊次数超过一次(129人,27%)。样本包括仅被诊断为高血压的患者(308人,64%)、仅患糖尿病的患者(45人,9%)以及同时患有高血压和糖尿病的患者(127人,26%)。
除了在遵守随访预约方面,失访组和随访组之间未观察到具有统计学意义的社会经济差异。在没有随访意识的患者中失访的可能性更高(比值比[OR]=2.5,95%置信区间[CI]:1.05 - 4.83),感到受辱的患者(OR = 15.51,95% CI:1.01 - 238.90),就诊的医疗机构医生仅在某些时间坐诊的患者(OR = 7.37,95% CI:1.07 - 50.61),就诊的医疗机构没有必要诊断设备的患者,认为NHIS对糖尿病诊断检查覆盖不足的患者,以及接受传统或草药治疗的患者(OR = 16.90,95% CI:3.12 - 91.45)。相反,来自阿散蒂地区的患者(OR = 0.58,95% CI:0.35 - 0.96)、接受过诊断程序教育的患者(OR = 0.28,95% CI:0.08 - 0.98)以及治疗未得到控制的患者(OR = 0.04,95% CI:0.00 - 0.69)失访的可能性较小。此外,十年前以上被诊断的患者(OR = 0.44,95% CI:0.24 - 0.79)以及对建立支持小组持中立态度的患者失访的可能性较小。
该研究发现,缺乏随访意识、受辱感以及对传统或草药治疗的偏好是高血压和糖尿病患者失访行为的关键驱动因素。因此,补救政策应包括加强患者对随访重要性的教育,确保基本药物、诊断设备和医生的可及性,扩大NHIA的财务覆盖范围,以及将传统医学纳入标准医疗保健以提高治疗依从性并降低失访率。