De la Torre Canales Giancarlo, Poluha Rodrigo Lorenzi, Soares Flávia Fonseca Carvalho, Ferreira Dyna Mara Araújo Oliveira, Sánchez-Ayala Alfonso, Bonjardim Leonardo Rigoldi, Ernberg Malin, Conti Paulo César Rodrigues
Department of Prosthodontics, Bauru Orofacial Pain Group, Bauru School of Dentistry, University of São Paulo, Sao Paulo, Brazil.
Division of Oral Rehabilitation, Department of Dental Medicine, Karolinska Institutet, Huddinge, Sweden.
J Headache Pain. 2025 May 6;26(1):98. doi: 10.1186/s10194-025-02055-7.
Resistance to treatments have been assessed in chronic conditions such as migraine, but not in temporomandibular disorders (TMD). This study aimed to identify factors that influence treatment outcome in patients with myofascial TMD pain.
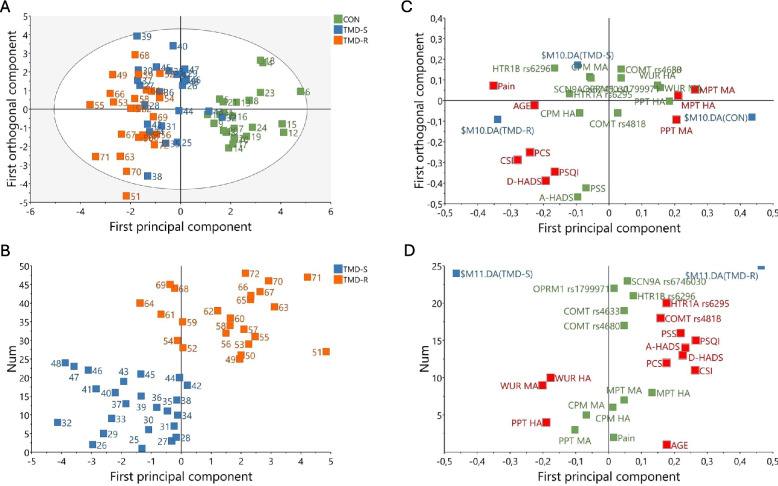
Seventy-two females were divided into three groups: TMD successfully treated (TMD-S, n = 24), TMD resistant to treatment (TMD-R, n = 24) and Controls without TMD (n = 24). Criteria for resistance included: less than 30% pain reduction after three months of conservative treatment and an average pain intensity > 50 mm (VAS) during the last month. Quantitative sensory testing (QST), psychosocial status and genetic polymorphisms were examined. ANOVA on ranks (psychosocial variables) with Dunn's test as post-hoc or ANOVA (age and somatosensory variables) with Tukey test as post-hoc test, and Dwass-Steel-Critchlow-Fligner test (genetic variables) were used for univariate groups comparisons. Multivariate statistics were used to identify outcomes that separated the groups.
QST assessment revealed lower baseline pressure pain threshold and higher wind-up ratio in the trigeminally and spinally innervated areas in the TMD-R group compared with the other groups (p = 0.01). Also, the TMD-R group presented higher values in all assessed psychosocial variables (p < 0.01) and higher prevalence of the HTR1A polymorphism rs6295 (p = 0.02) compared with the other groups at baseline. Multivariate analysis showed that the three variables that distinguished the best between TMD-R and TMD-S were sleeping quality, central sensitization, and depressive symptoms.
Psychosocial, somatosensory, and genetic alterations are related to unsuccessful treatment response in myofascial TMD patients.
在偏头痛等慢性疾病中已对治疗抵抗情况进行了评估,但在颞下颌关节紊乱病(TMD)中尚未进行评估。本研究旨在确定影响肌筋膜性TMD疼痛患者治疗结果的因素。
72名女性被分为三组:TMD成功治疗组(TMD-S,n = 24)、TMD治疗抵抗组(TMD-R,n = 24)和无TMD的对照组(n = 24)。治疗抵抗的标准包括:保守治疗三个月后疼痛减轻少于30%,且在最后一个月平均疼痛强度>50mm(视觉模拟评分法)。对定量感觉测试(QST)、心理社会状况和基因多态性进行了检查。使用秩和检验(心理社会变量)及Dunn检验作为事后检验,或使用方差分析(年龄和躯体感觉变量)及Tukey检验作为事后检验,以及Dwass-Steel-Critchlow-Fligner检验(基因变量)进行单变量组间比较。使用多变量统计来确定区分各组的结果。
QST评估显示,与其他组相比,TMD-R组在三叉神经和脊髓支配区域的基线压力疼痛阈值较低,痛觉过敏率较高(p = 0.01)。此外,与其他组相比,TMD-R组在所有评估的心理社会变量中数值更高(p < 0.01),且在基线时HTR1A基因多态性rs6295的患病率更高(p = 0.02)。多变量分析表明,在TMD-R组和TMD-S组之间区分效果最佳的三个变量是睡眠质量、中枢敏化和抑郁症状。
心理社会、躯体感觉和基因改变与肌筋膜性TMD患者治疗反应不佳有关。