Li Mian, Xu Min, Ding Yi, Lin Hong, Qin Guijun, Wang Tiange, Xu Yu, Chen Yuhong, Wang Shuangyuan, Zhao Zhiyun, Zheng Jie, Yan Li, Shi Lixin, Gao Zhengnan, Chen Lulu, Zeng Tianshu, Hu Ruying, Ye Zhen, Yu Xuefeng, Chen Gang, Su Qing, Mu Yiming, Tang Xulei, Wan Qin, Wang Guixia, Shen Feixia, Gu Xuejiang, Luo Zuojie, Qin Yingfen, Chen Li, Hou Xinguo, Huo Yanan, Li Qiang, Qiao Hong, Zhang Yinfei, Liu Chao, Wang Youmin, Wu Shengli, Yang Tao, Deng Huacong, Zhao Jiajun, Ning Guang, Lu Jieli, Wang Weiqing, Bi Yufang
Department of Endocrine and Metabolic Diseases, Shanghai Institute of Endocrine and Metabolic Diseases, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, 197 Rui-Jin 2nd Road, Shanghai, 200025, China.
Shanghai National Clinical Research Center for metabolic Diseases, Key Laboratory for Endocrine and Metabolic Diseases of the National Health Commission of the PR China, Shanghai Key Laboratory for Endocrine Tumor, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China.
Cardiovasc Diabetol. 2025 May 9;24(1):197. doi: 10.1186/s12933-025-02735-3.
Definition and staging rationale of cardiovascular-kidney-metabolic syndrome were developed. The utility of cardiovascular-kidney-metabolic construct in risk stratification and target strategies of health and behavior modifications needs to be addressed. The study aims to investigate the individual and combined associations of cardiovascular-kidney-metabolic stage and cardiovascular health (CVH) by Life's Essential 8 (LE 8) with incident cardiovascular events (CVD), and determine the distribution and contribution of domain-specific CVH across cardiovascular-kidney-metabolic stages.
The study included 100,727 individuals in the China Cardiovascular Disease and Cancer Cohort with complete data on cardiovascular-kidney-metabolic factors and LE 8 metrics, with a median follow-up of 10.1 years. Cardiovascular-kidney-metabolic stages and CVH metrics (nicotine exposure, diet, physical activity, sleep, body mass index, blood lipids, blood pressure, blood glucose) were defined according to Presidential Advisory from the American Heart Association. Incident CVD events including cardiovascular death, myocardial infarction, and stroke were validated. The Fine-Gray hazard model was used to calculate hazard ratios (HRs) and 95% confidence intervals (CIs) of CKM stages or CVH status associated with CVD.
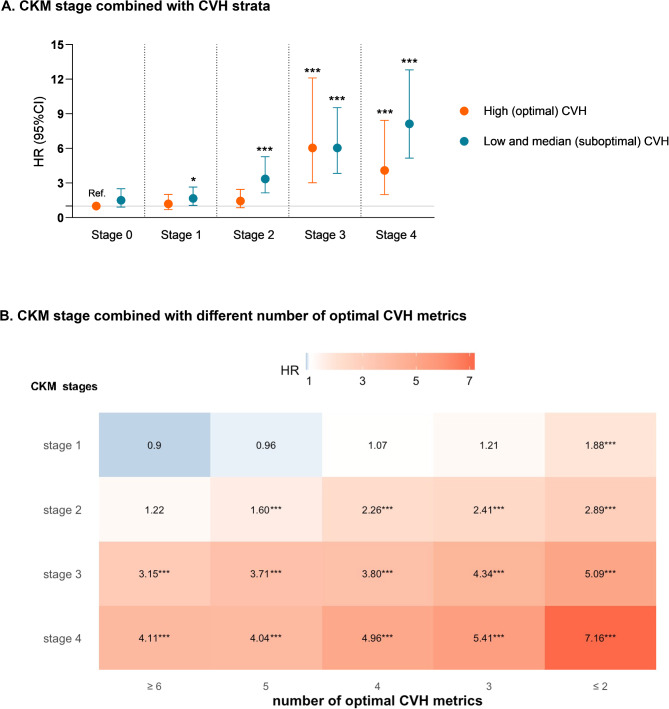
Compared with cardiovascular-kidney-metabolic stage 0, the adjusted competing HRs and 95% CIs of CVD events were 1.20 (0.95-1.51), 2.45 (1.97-3.04), 4.43 (3.53-5.58), and 5.95 (4.75-7.45) from stage 1 to stage 4, respectively. Optimal CVH status and each optimal CVH metric presented a significantly decreased risk of CVD events. Variation was observed in the association between cardiovascular-kidney-metabolic stage and CVD events with different CVH status or numbers of optimal CVH metrics. Compared with those in stage 0, Participants in stage 1 or 2 with optimal CVH no longer had elevated risks for incident CVD events. Suboptimal health factor contributed larger population attributable fractions to CVD events in cardiovascular-kidney-metabolic stage 0-2 (51.2%) than in stage 3-4 (25.2%), whereas suboptimal health behavior exhibited larger contribution in advanced stages (13.1% in stage 0-2 and 18.2% in stage 3-4).
The study indicated that cardiovascular-kidney-metabolic stage was associated with cardiovascular events, and optimal cardiovascular health could attenuate this risk. Health factor contributed predominantly at the early-stage, whereas health behavior exhibited consistent and slightly increased contribution along the spectrum. These findings support the utility of cardiovascular-kidney-metabolic construct and highlight the importance of target health improvement based on LE 8 framework.
制定了心血管-肾脏-代谢综合征的定义和分期依据。心血管-肾脏-代谢结构在风险分层以及健康和行为改变目标策略中的效用有待探讨。本研究旨在调查心血管-肾脏-代谢分期与基于生命八大要素(LE 8)的心血管健康(CVH)与心血管事件(CVD)发生之间的个体及联合关联,并确定特定领域的CVH在心血管-肾脏-代谢各阶段的分布及贡献。
本研究纳入了中国心血管疾病与癌症队列中的100,727名个体,这些个体拥有关于心血管-肾脏-代谢因素和LE 8指标的完整数据,中位随访时间为10.1年。心血管-肾脏-代谢分期和CVH指标(尼古丁暴露、饮食、身体活动、睡眠、体重指数、血脂、血压、血糖)根据美国心脏协会的总统咨询意见进行定义。对包括心血管死亡、心肌梗死和中风在内的心血管疾病事件进行了验证。采用Fine-Gray风险模型计算与心血管疾病相关的心血管-肾脏-代谢分期或CVH状态的风险比(HRs)和95%置信区间(CIs)。
与心血管-肾脏-代谢0期相比,心血管疾病事件的校正竞争风险比及95%置信区间在1期至4期分别为1.20(0.95 - 1.51)、2.45(1.97 - 3.04)、4.43(3.53 - 5.58)和5.95(4.75 - 7.45)。最佳CVH状态及每个最佳CVH指标均显示心血管疾病事件风险显著降低。在不同CVH状态或最佳CVH指标数量下,观察到心血管-肾脏-代谢分期与心血管疾病事件之间关联存在差异。与0期参与者相比,处于1期或2期且CVH最佳的参与者发生心血管疾病事件的风险不再升高。在心血管-肾脏-代谢0 - 2期,次优健康因素对心血管疾病事件的人群归因分数(51.2%)高于3 - 4期(25.2%),而次优健康行为在晚期的贡献更大(0 - 2期为13.1%,3 - 4期为18.2%)。
该研究表明心血管-肾脏-代谢分期与心血管事件相关,最佳心血管健康可降低此风险。健康因素在早期起主要作用,而健康行为在整个过程中贡献持续且略有增加。这些发现支持了心血管-肾脏-代谢结构的效用,并突出了基于LE 8框架进行目标健康改善的重要性。