Wang Liang, Sun Yilan, Sang Qing, Wang Zheng, Yu Chengyuan, Li Zhehong, Shang Mingyue, Zhang Nengwei, Du Dexiao
Surgery Centre of Diabetes Mellitus, Capital Medical University Affiliated Beijing Shijitan Hospital, Beijing, 100038, People's Republic of China.
Diabetes Metab Syndr Obes. 2025 May 7;18:1467-1487. doi: 10.2147/DMSO.S508067. eCollection 2025.
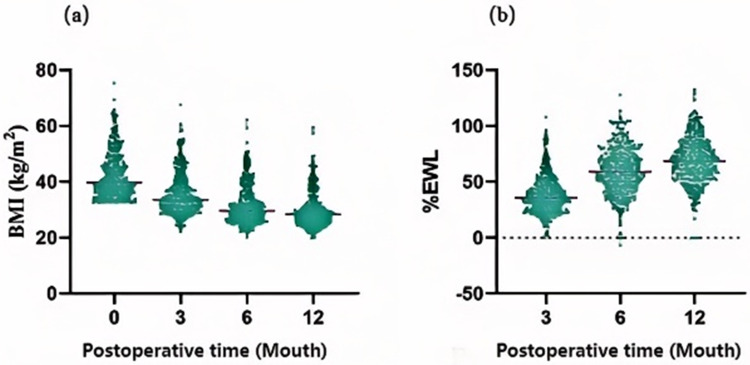
Laparoscopic sleeve gastrectomy (LSG) is associated with sustained and substantial weight loss. However, suboptimal results are observed in certain patients.
Drawing from body composition data at our center, clinically accessible predictive factors for weight loss outcomes were identified, leading to the development and validation of a preoperative predictive model for weight loss following LSG.
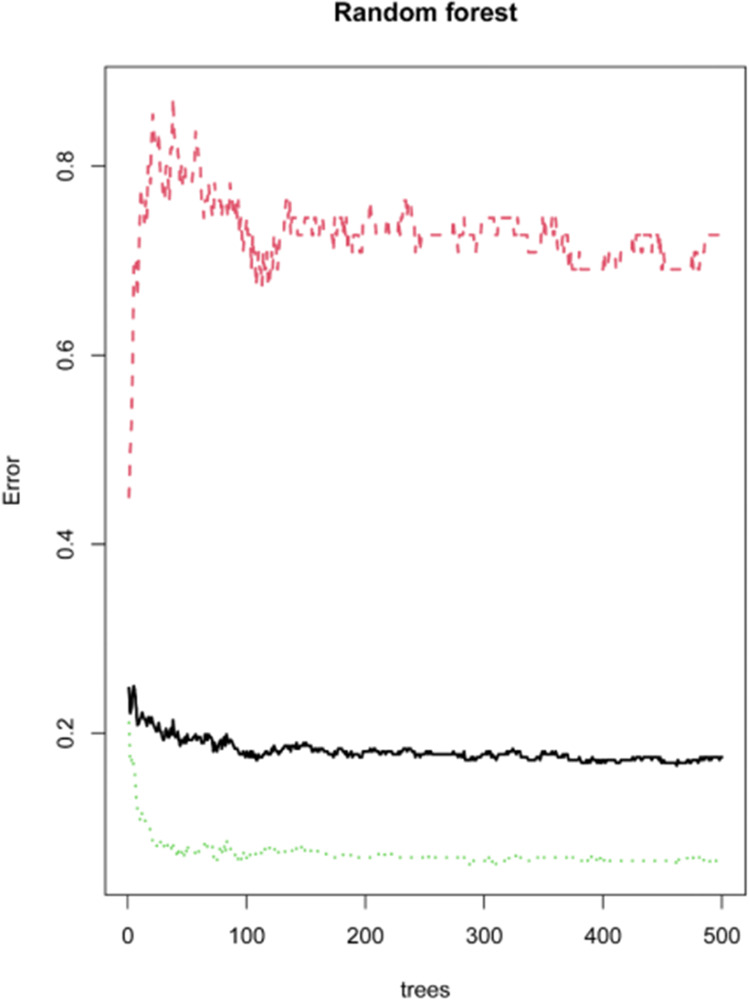
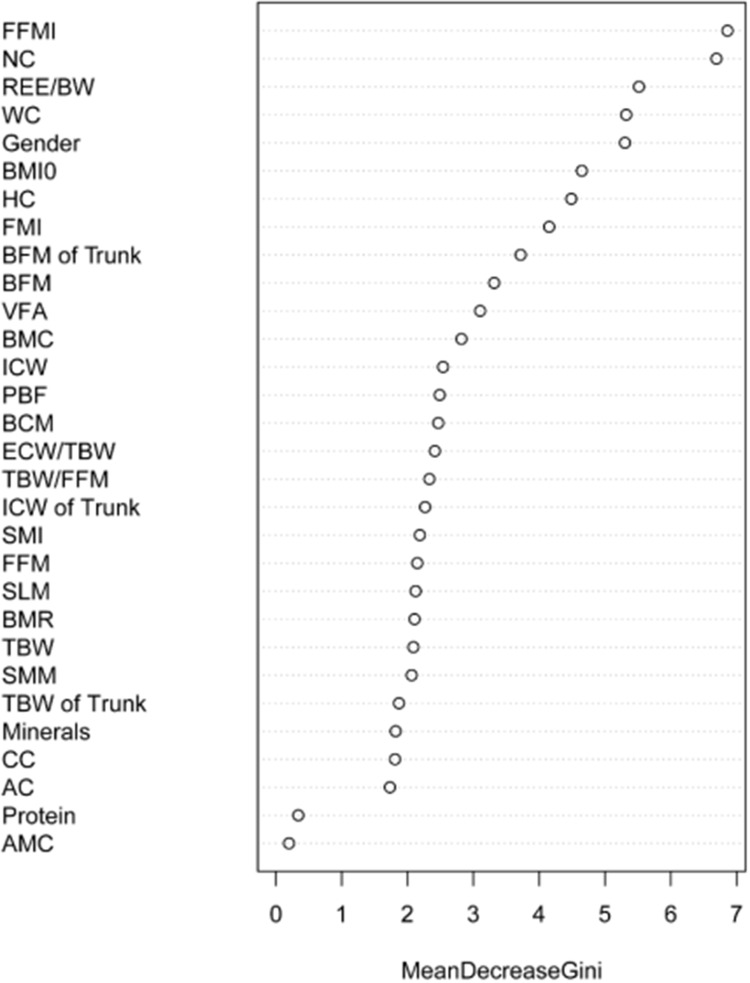
A retrospective analysis was conducted on the general clinical baseline and body composition data of obese patients (body mass index [BMI] ≥ 32.5 kg/m) who underwent LSG between December 2016 and December 2022. Independent predictors for weight loss outcomes were selected through univariate logistic regression, random forest analysis, and multivariate logistic regression. Subsequently, a nomogram was developed to predict weight loss outcomes and was evaluated for discrimination, accuracy, and clinical utility, with validation performed in a separate cohort.
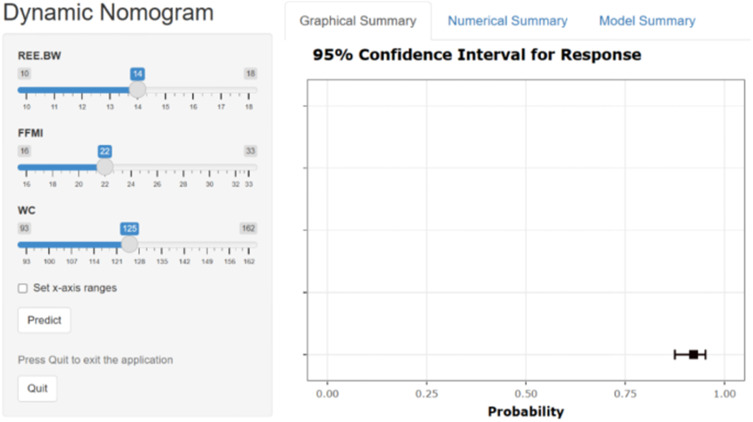
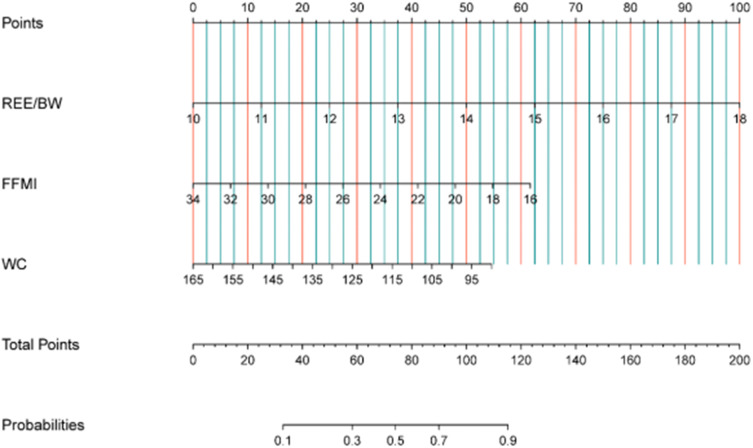
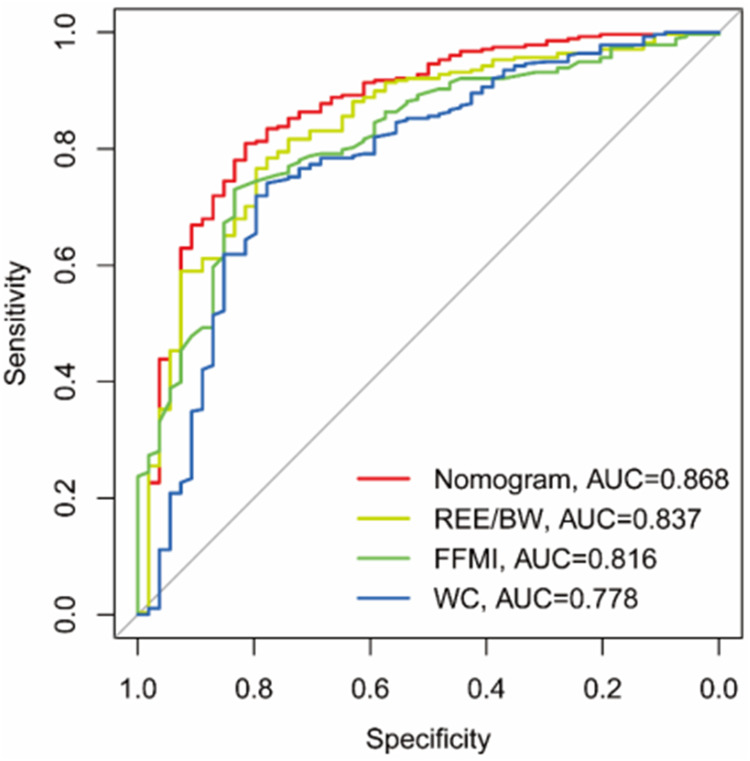
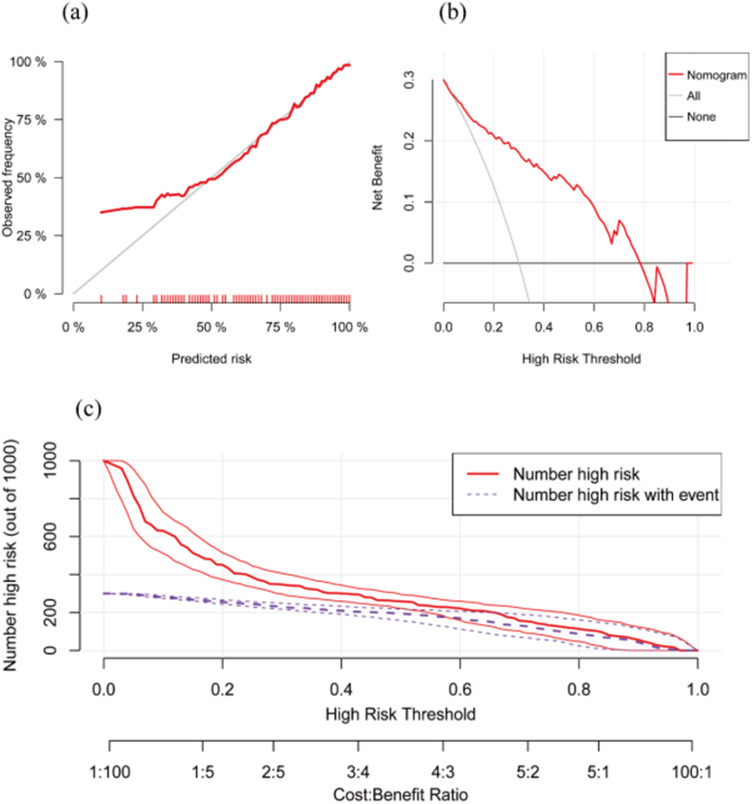
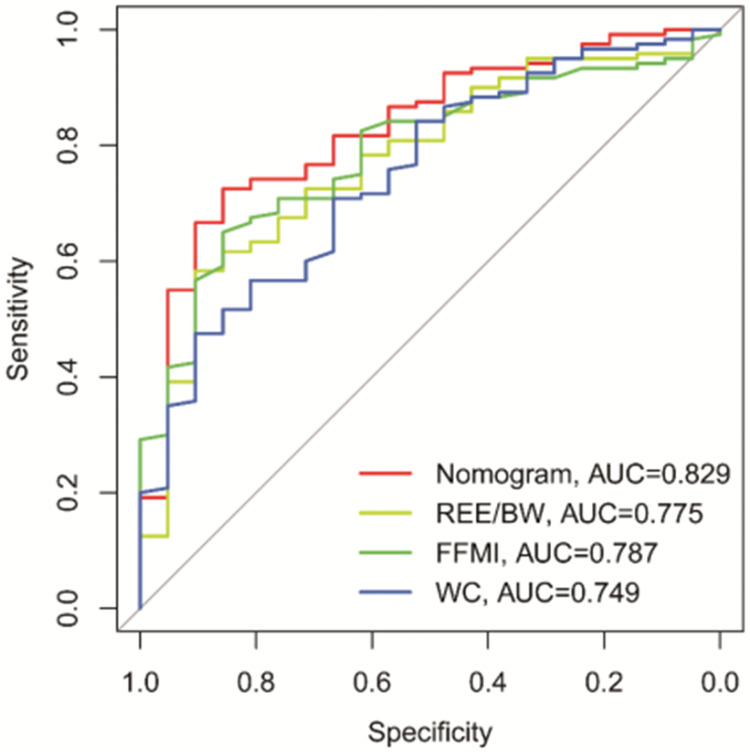
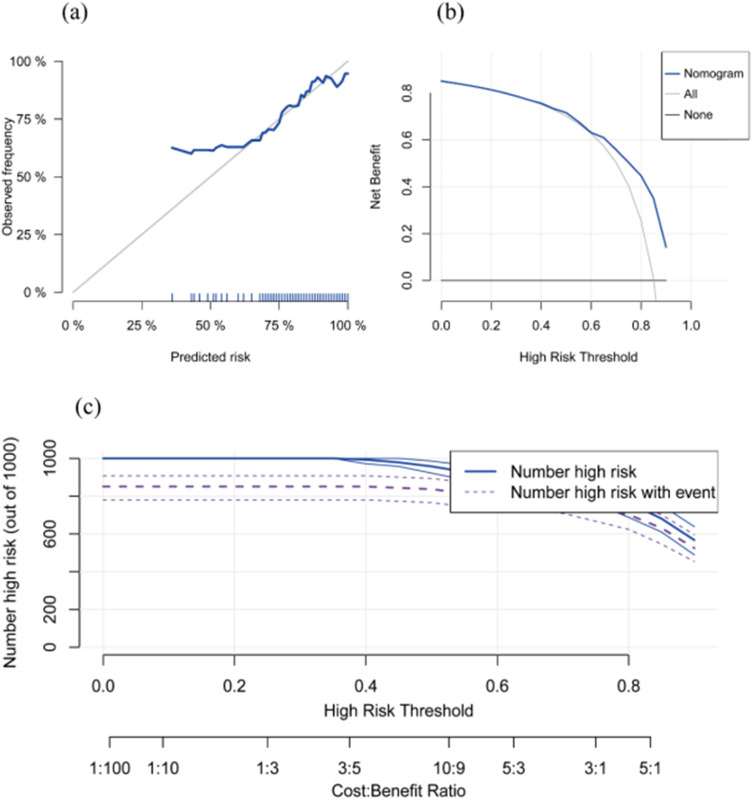
A total of 473 patients with mean BMI were included. The preoperative resting energy expenditure to body weight ratio (REE/BW), fat-free mass index (FFMI), and waist circumference (WC) emerged as independent predictive factors for weight loss outcomes at one year post-LSG. These body composition parameters were incorporated into the construction of an Inbody predictive nomogram, which yielded area under the curve (AUC) values of 0.868 (95% CI: 0.826-0.902) for the modeling cohort and 0.829 (95% CI: 0.756-0.887) for the validation cohort. Calibration curves, decision curve analysis (DCA), and clinical impact curves (CIC) from both groups demonstrated the model's robust discrimination, accuracy, and clinical utility.
In obese Chinese patients with a BMI ≥ 32.5 kg/m, the Inbody-based nomogram integrating REE/BW, FFMI, and WC offers an effective preoperative tool for predicting weight loss outcomes one year after LSG, facilitating surgical planning and postoperative management.
腹腔镜袖状胃切除术(LSG)与持续且显著的体重减轻相关。然而,在某些患者中观察到效果欠佳的情况。
根据我们中心的身体成分数据,确定临床上可获取的体重减轻结果预测因素,从而开发并验证LSG术后体重减轻的术前预测模型。
对2016年12月至2022年12月期间接受LSG的肥胖患者(体重指数[BMI]≥32.5kg/m²)的一般临床基线和身体成分数据进行回顾性分析。通过单因素逻辑回归、随机森林分析和多因素逻辑回归选择体重减轻结果的独立预测因素。随后,开发了一种列线图来预测体重减轻结果,并对其区分度、准确性和临床实用性进行评估,在一个单独的队列中进行验证。
共纳入473例平均BMI的患者。术前静息能量消耗与体重比(REE/BW)、去脂体重指数(FFMI)和腰围(WC)成为LSG术后一年体重减轻结果的独立预测因素。这些身体成分参数被纳入Inbody预测列线图的构建中,该列线图在建模队列中的曲线下面积(AUC)值为0.868(95%CI:0.826-0.902),在验证队列中的AUC值为0.829(95%CI:0.756-0.887)。两组的校准曲线、决策曲线分析(DCA)和临床影响曲线(CIC)均表明该模型具有强大的区分度、准确性和临床实用性。
在BMI≥32.5kg/m²的肥胖中国患者中,整合REE/BW、FFMI和WC的基于Inbody的列线图为预测LSG术后一年的体重减轻结果提供了一种有效的术前工具,有助于手术规划和术后管理。