Ceolin Chiara, Sella Stefania, Simonato Cristina, Bukli Ester, Bano Giulia, Camozzi Valentina, Bertocco Anna, Torres Marco Onofrio, Cecchinato Alberta, Diogo Martin, Peleg Falb Mor, Guidolin Francesca, Rodà Maria Grazia, Cannito Michele, Berizzi Antonio, Venturin Andrea, Cianci Vito, Pala Elisa, Cerchiaro Mariachiara, Boemo Deris Gianni, Nesoti Maria Vittoria, Arcidiacono Gaetano Paride, Simioni Paolo, Ruggieri Pietro, Sergi Giuseppe, Giannini Sandro, De Rui Marina
Geriatrics Division, Department of Medicine, University of Padua, Padua, Italy.
Department of Neurobiology, Care Sciences and Society, Karolinska Institutet and Stockholm University, Aging Research Center, Stockholm, Sweden.
BMC Geriatr. 2025 May 14;25(1):338. doi: 10.1186/s12877-025-06009-1.
Osteoporosis is a chronic condition characterized by increased fracture risk. Fragility fractures, especially hip fractures, represent a significant health and economic burden due to population aging. Despite the efficacy of approved treatments in lowering fracture recurrence, post-fracture treatment rates remain suboptimal. To address these issues, various post-fracture care programs, including Fracture Liaison Services (FLS), have been implemented worldwide. While FLS models effectively reduce refracture risk and maintain cost-effectiveness, it is unclear if these benefits apply equally to all patients, especially those with higher comorbidities and reduced functional capacity, who may face worse prognoses. This study aimed to identify the primary factors influencing anti-fracture therapy decisions in older patients with fragility fractures, using a multidimensional geriatric assessment approach integrated into our FLS program.
A retrospective analysis was conducted on patients aged 65 and above with hip fractures admitted to Azienda Ospedale-Università Padova. Patients were categorized based on anti-fracture treatment (bisphosphonates, Denosumab, anabolic agents) or calcium/vitamin D supplements only. Clinical data, including the Multidimensional Prognostic Index (MPI) and its components, were collected. Statistical comparisons between treated and untreated groups were made, and a CHAID decision tree was used to explore decision-influencing factors.
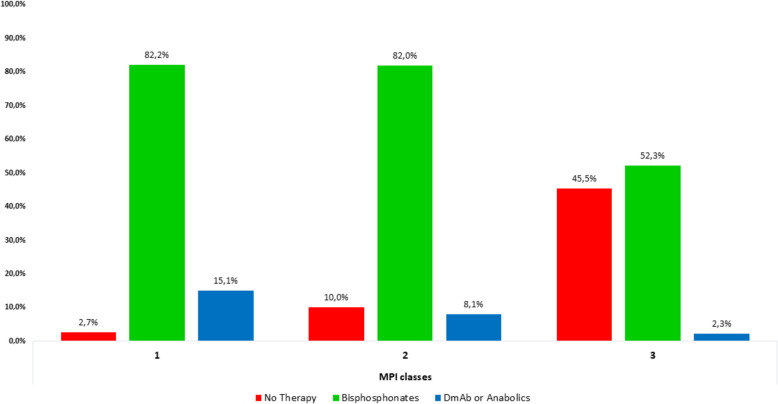
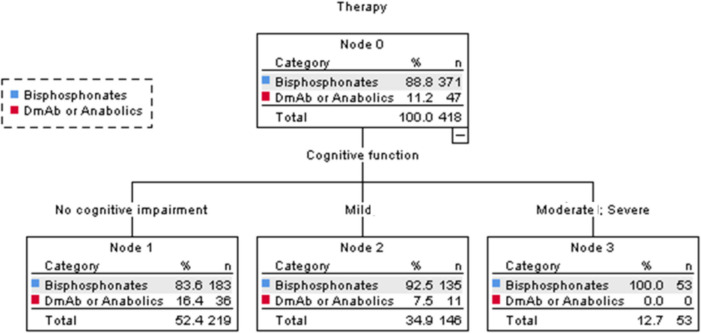
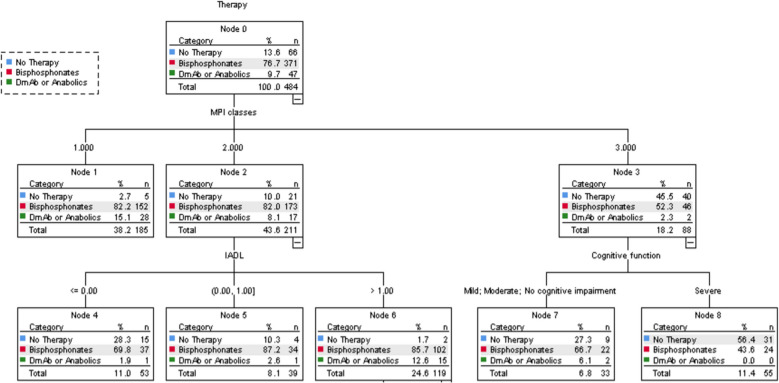
The study included 493 patients (average age 84.7 years, 71.8% female). Patients receiving anti-fracture treatment were notably younger, with only 11.2% classified as MPI class 3 (severe prognosis) compared to 60.8% of untreated patients (p < 0.001). Among treated patients (n = 427), 75.3% received bisphosphonates, 7.3% Denosumab, and 2.2% anabolic agents. The CHAID decision tree highlighted MPI class as the primary determinant of treatment, with functional autonomy (Instrumental Activity of Daily Living or IADL) and cognitive status as subsequent factors, leading to an overall prediction accuracy of 70%.
The integration of the MPI into multidisciplinary taking care of old patients with hip fractures may provide a structured approach for individualizing treatment decisions, considering aspects such as prognosis, functional autonomy, and cognitive status. Further studies are needed to validate the long-term outcomes of this approach.
骨质疏松症是一种以骨折风险增加为特征的慢性疾病。由于人口老龄化,脆性骨折,尤其是髋部骨折,带来了重大的健康和经济负担。尽管已批准的治疗方法在降低骨折复发方面有效,但骨折后的治疗率仍不理想。为解决这些问题,包括骨折联络服务(FLS)在内的各种骨折后护理计划已在全球范围内实施。虽然FLS模式有效降低了再骨折风险并保持了成本效益,但尚不清楚这些益处是否同样适用于所有患者,尤其是那些合并症较多且功能能力下降、预后可能更差的患者。本研究旨在使用纳入我们FLS计划的多维老年评估方法,确定影响老年脆性骨折患者抗骨折治疗决策的主要因素。
对帕多瓦大学医院收治的65岁及以上髋部骨折患者进行回顾性分析。患者根据抗骨折治疗(双膦酸盐、地诺单抗、促合成代谢药物)或仅补充钙/维生素D进行分类。收集临床数据,包括多维预后指数(MPI)及其组成部分。对治疗组和未治疗组进行统计学比较,并使用CHAID决策树探索决策影响因素。
该研究纳入了493例患者(平均年龄84.7岁,71.8%为女性)。接受抗骨折治疗的患者明显更年轻,只有11.2%被归类为MPI 3级(严重预后),而未治疗患者为60.8%(p<0.001)。在接受治疗的患者(n = 427)中,75.3%接受双膦酸盐治疗,7.3%接受地诺单抗治疗,2.2%接受促合成代谢药物治疗。CHAID决策树突出显示MPI分级是治疗的主要决定因素,随后是功能自主性(日常生活工具性活动或IADL)和认知状态,总体预测准确率为70%。
将MPI纳入老年髋部骨折患者的多学科护理中,可能会提供一种结构化方法,用于根据预后、功能自主性和认知状态等方面,为治疗决策个体化。需要进一步研究来验证这种方法的长期效果。