Zheng Yumin, Lu Xingyu, Dong Huijing, Li Jia, Shen Yulei, Liu Zhening, Cui Huijuan
Graduate School, Beijing University of Chinese Medicine, Beijing 100029, P.R. China.
Department of Oncology, Affiliated Hospital of Shandong University of Traditional Chinese Medicine, Jinan, Shandong 250011, P.R. China.
Oncol Lett. 2025 May 2;30(1):328. doi: 10.3892/ol.2025.15074. eCollection 2025 Jul.
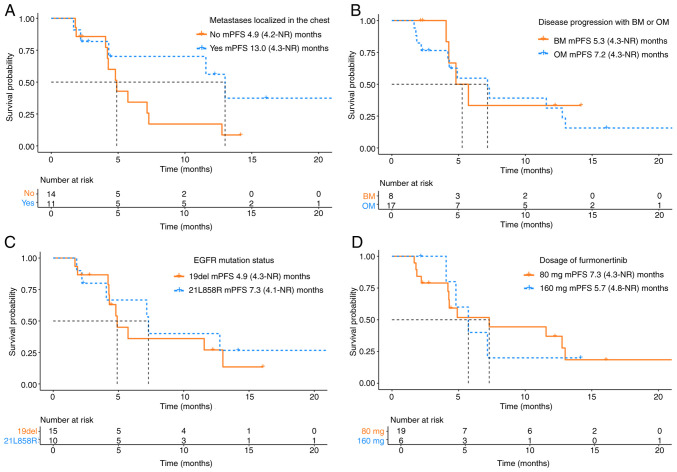
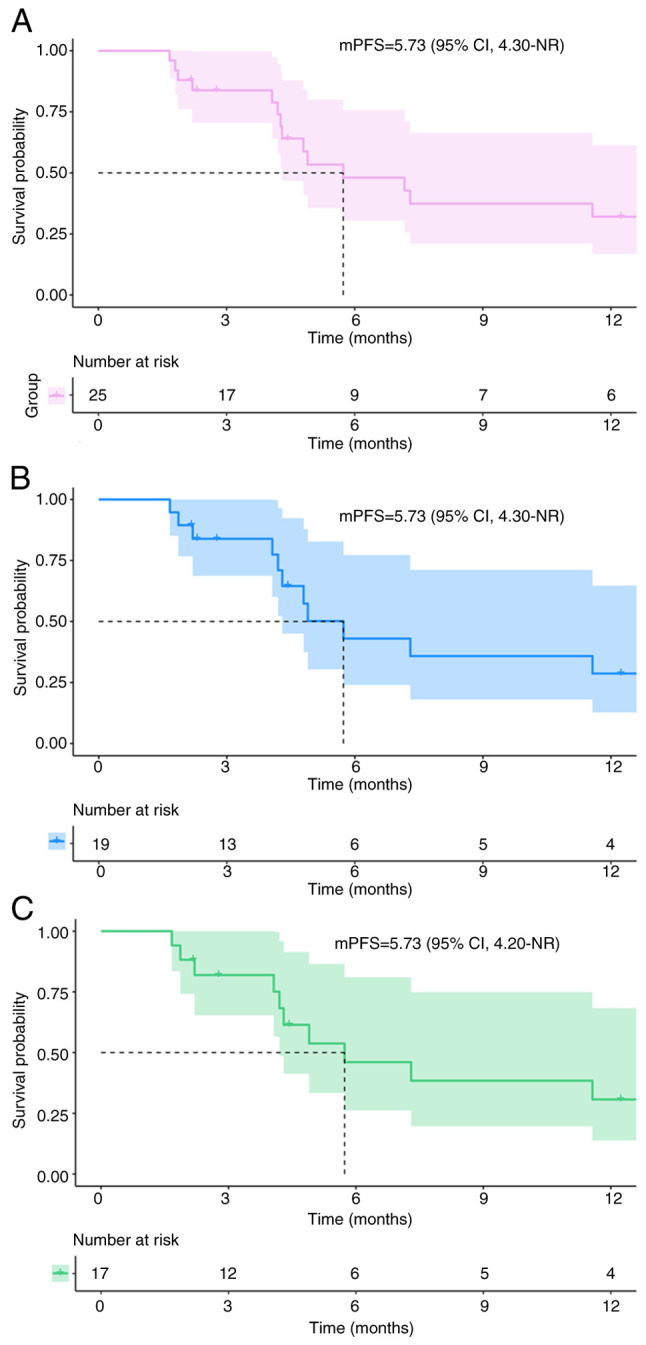
Currently, treatments for patients with non-small cell lung cancer harboring epidermal growth factor receptor (EGFR) mutations are limited after receiving multiple lines of therapy. Furmonertinib, a newly developed third-generation EGFR-tyrosine kinase inhibitor (TKI), has shown potential as a subsequent treatment. To explore efficacy and safety of furmonertinib, the present retrospective study analyzed patients with EGFR-mutant advanced lung adenocarcinoma (LUAD) who received furmonertinib after the failure of multiple lines of therapy at the China-Japan Friendship Hospital (Beijing, China) between December 2021 and April 2024. Data on patient demographics, treatment efficacy and safety outcomes were assessed until disease progression. A total of 25 patients with advanced LUAD were retrospectively included in the analysis. Among them, 15 (60.0%) harbored exon 19del, whilst 10 (40.0%) had exon21 L858R mutations. Pre-treatment genetic testing was performed in 14 patients (56.0%). Prior to furmonertinib therapy, 17, 5 and 19 patients had previously received first-, second- and third-generation EGFR-TKIs, respectively. The median line of treatment before furmonertinib was 3. The median progression-free survival was 5.73 (95% confidence interval, 4.30-not reached) months. The objective response rate was 16.0% (n=4) and the disease control rate was 88.0% (n=22). A total of 18 (72.0%) patients experienced at least one adverse event (AE). The rate of AEs was 80.0% (n=20) for grade 1-2, and 20.0% (n=5) for grade 3-4 AEs. No AEs led to treatment discontinuation, dose reductions or death. In conclusion, furmonertinib is a viable treatment option for patients with EGFR-mutant advanced LUAD after the failure of multiple lines of therapy, even after resistance to treatment with third-generation EGFR-TKIs targeted agents. However, further large-scale clinical studies are warranted to validate these findings.
目前,对于携带表皮生长因子受体(EGFR)突变的非小细胞肺癌患者,在接受多线治疗后,治疗方案有限。伏美替尼是一种新开发的第三代EGFR酪氨酸激酶抑制剂(TKI),已显示出作为后续治疗的潜力。为了探究伏美替尼的疗效和安全性,本回顾性研究分析了2021年12月至2024年4月期间在中国-日本友好医院(北京,中国)接受多线治疗失败后接受伏美替尼治疗的EGFR突变型晚期肺腺癌(LUAD)患者。评估患者人口统计学、治疗疗效和安全性结果的数据直至疾病进展。共有25例晚期LUAD患者被纳入回顾性分析。其中,15例(60.0%)携带19号外显子缺失,而10例(40.0%)有21号外显子L858R突变。14例患者(56.0%)进行了治疗前基因检测。在伏美替尼治疗前,分别有17例、5例和19例患者曾接受过第一代、第二代和第三代EGFR-TKIs治疗。伏美替尼治疗前的中位治疗线数为3。中位无进展生存期为5.73(95%置信区间,4.30-未达到)个月。客观缓解率为16.0%(n = 4),疾病控制率为88.0%(n = 22)。共有18例(72.0%)患者经历了至少一次不良事件(AE)。1-2级AE的发生率为80.0%(n = 20),3-4级AE的发生率为20.0%(n = 5)。没有AE导致治疗中断、剂量减少或死亡。总之,对于多线治疗失败后的EGFR突变型晚期LUAD患者,即使在对第三代EGFR-TKIs靶向药物治疗耐药后,伏美替尼也是一种可行的治疗选择。然而,需要进一步的大规模临床研究来验证这些发现。