Wu Liyan, Zhang Ye, Gu Li, Wang Junyu, Wei Bing, Liu Yugeng
Department of Infectious Diseases and Clinical Microbiology, Beijing Chaoyang Hospital, Capital Medical University, Beijing, 100043, People's Republic of China.
Emergency Medicine Clinical Research Center, Beijing Chaoyang Hospital, Capital Medical University, & Beijing Key Laboratory of Cardiopulmonary Cerebral Resuscitation, Clinical Center for Medicine in Acute Infection, Capital Medical University, Beijing, 100043, People's Republic of China.
Int J Gen Med. 2025 May 9;18:2477-2486. doi: 10.2147/IJGM.S512295. eCollection 2025.
Identification of prognostic biomarkers for critical illness are essential to improving mortality in the context of precision medicine. The purpose of this study was to evaluate the prognostic value of interleukin-6 (IL-6) and platelet-derived growth factor AA(PDGF-AA) in predicting 28-day mortality in critically ill patients.
199 critically ill patients were recruited from the emergency department of the Beijing Chaoyang Hospital, Capital Medical University, between October 2020 and April 2021. IL-6, PDGF-AA and other markers were tested immediately, and the Sequential Organ Failure Assessment (SOFA) and Acute Physiology and Chronic Health Evaluation II (APACHE II) scores were calculated within 24h of admission to the emergency department. Patients were divided into survival and non-survival groups according to clinical outcomes for 28 days. The quantitative detections of IL-6 and PDGF-AA were performed using the Luminex assay. Spearman correlation, logistic regression, and receiver operating characteristic curve (ROC) analyses were conducted for comparison.
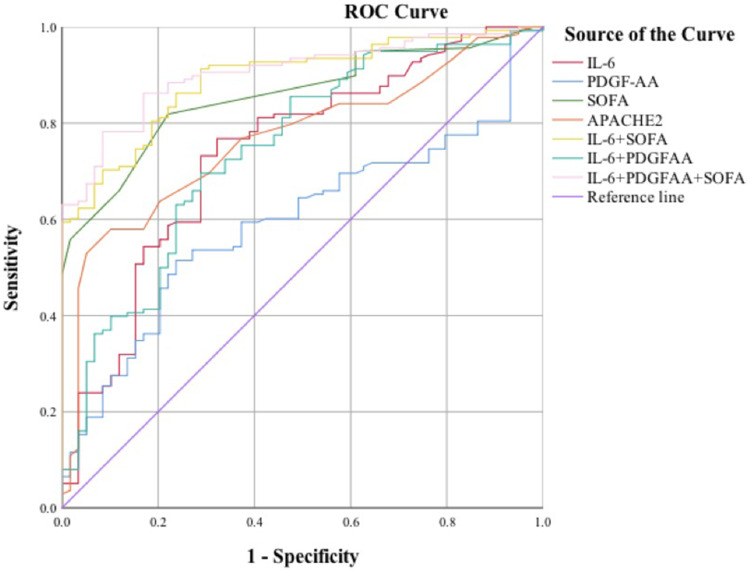
Among 199 patients, 139 died and 60 survived within 28 days, IL-6 and PDGF-AA levels were higher in the non-survival group (P<0.05). IL-6 levels correlated with PDGF-AA levels in the non-survival group (P<0.001). IL-6 and PDGF-AA were independent predictors off 28-day mortality in critically ill patients (OR=1.003, 1.002). Combination of IL-6 and SOFA can make an AUROC of 0.892 with a specificity of 91.4%. Combination of IL-6, PDGF-AA and SOFA can make an AUROC of 0.905 with a specificity of 91.5%.
This study highlights the importance of monitoring serum levels of IL-6 and PDGF-AA in critically ill patients. Compared with the marker alone, combinations with other conventional risk factors have better predictive values.
识别危重症的预后生物标志物对于在精准医疗背景下提高死亡率至关重要。本研究的目的是评估白细胞介素-6(IL-6)和血小板衍生生长因子AA(PDGF-AA)在预测危重症患者28天死亡率方面的预后价值。
2020年10月至2021年4月期间,从首都医科大学附属北京朝阳医院急诊科招募了199例危重症患者。立即检测IL-6、PDGF-AA和其他标志物,并在急诊科入院后24小时内计算序贯器官衰竭评估(SOFA)和急性生理与慢性健康状况评估II(APACHE II)评分。根据28天的临床结局将患者分为存活组和非存活组。使用Luminex测定法对IL-6和PDGF-AA进行定量检测。进行Spearman相关性、逻辑回归和受试者工作特征曲线(ROC)分析以进行比较。
在199例患者中,139例在28天内死亡,60例存活,非存活组的IL-6和PDGF-AA水平较高(P<0.05)。非存活组中IL-6水平与PDGF-AA水平相关(P<0.001)。IL-6和PDGF-AA是危重症患者28天死亡率的独立预测因素(OR=1.003,1.002)。IL-6与SOFA联合可使曲线下面积(AUROC)为0.892,特异性为91.4%。IL-6、PDGF-AA与SOFA联合可使AUROC为0.905,特异性为91.5%。
本研究强调了监测危重症患者血清IL-6和PDGF-AA水平的重要性。与单独的标志物相比,与其他传统危险因素联合具有更好的预测价值。