Ha Tuan Manh, Tran Man Minh, Le Tung Viet, Phung Nguyen The Nguyen
University of Medicine and Pharmacy at Ho Chi Minh City, Ho Chi Minh City, Vietnam; University Medical Center Ho Chi Minh City, Ho Chi Minh City, Vietnam.
University of Medicine and Pharmacy at Ho Chi Minh City, Ho Chi Minh City, Vietnam; City Children's Hospital, Ho Chi Minh City, Vietnam.
J Pediatr (Rio J). 2025 Jul-Aug;101(4):634-641. doi: 10.1016/j.jped.2025.04.006. Epub 2025 May 17.
This study aimed to evaluate the validity of models using Procalcitonin (PCT) alone and PCT combined with other biomarkers to predict early infection after pediatric open-heart surgery with cardiopulmonary bypass (CPB).
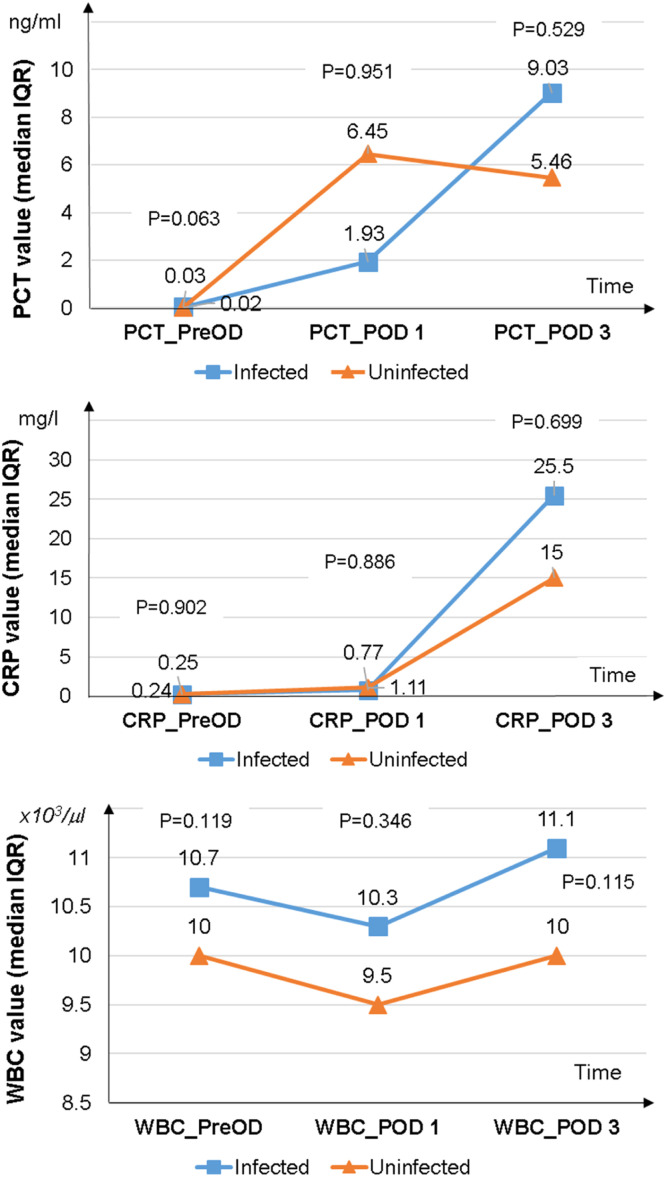
A prospective observational study was conducted on children undergoing open-heart surgery with CPB, without preoperative infection. Procalcitonin, C-reactive protein (CRP), and white blood cell (WBC) count were measured preoperatively and on postoperative days 1 and 3. Postoperative infection was defined according to the Centers for Disease Control and Prevention 2008 criteria.
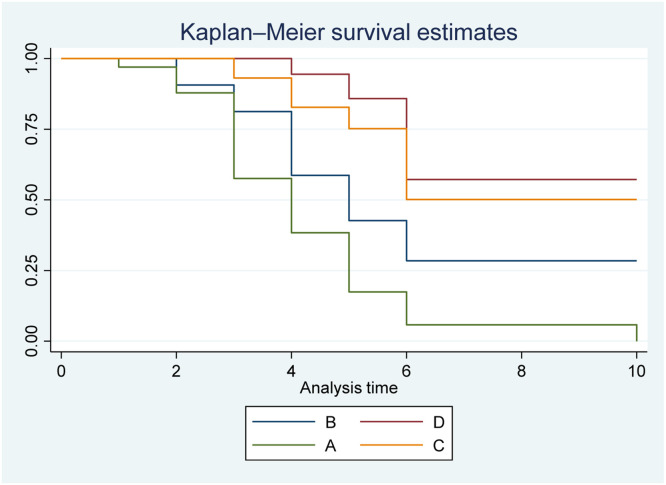
Fifty eligible cases were included, comprising 46 % males with a median age of 7 months (4-17). The AUC (area under the curve) for PCT on postoperative day 3 was 0.67 (0.51-0.82) (p = 0.085). The AUCs for the models combining PCT + CRP and PCT + WBC were 0.71 (0.57-0.86) (p = 0.014) and 0.72 (0.55-0.86) (p = 0.014), respectively. The AUC for the model combining PCT + CRP + WBC was 0.81 (0.69-0.93) (p = 0.002). The combination of PCT > 4.15 ng/ml, CRP > 22.03 mg/l, and WBC > 15.3 × 10/µl predicted infection with a hazard ratio 9.66 times (2.94-31.72) higher than PCT > 4.15 ng/ml alone (p < 0.05).
PCT measurement on the third postoperative day alone cannot predict infection in pediatric open-heart surgery with CPB. The combination of PCT with CRP and WBC may enhance early infection prediction, although further validation in larger, multicenter cohorts is warranted.
本研究旨在评估单独使用降钙素原(PCT)以及PCT与其他生物标志物联合使用的模型预测小儿体外循环心脏直视手术后早期感染的有效性。
对接受体外循环心脏直视手术且无术前感染的儿童进行前瞻性观察研究。术前以及术后第1天和第3天测量降钙素原、C反应蛋白(CRP)和白细胞(WBC)计数。术后感染根据疾病控制与预防中心2008年标准定义。
纳入50例符合条件的病例,其中46%为男性,中位年龄7个月(4 - 17个月)。术后第3天PCT的曲线下面积(AUC)为0.67(0.51 - 0.82)(p = 0.085)。PCT + CRP和PCT + WBC联合模型的AUC分别为0.71(0.57 - 0.86)(p = 0.014)和0.72(0.55 - 0.86)(p = 0.014)。PCT + CRP + WBC联合模型的AUC为0.81(0.69 - 0.93)(p = 0.002)。PCT > 4.15 ng/ml、CRP > 22.03 mg/l和WBC > 15.3×10⁹/µl联合预测感染的风险比是单独PCT > 4.15 ng/ml的9.66倍(2.94 - 31.72)(p < 0.05)。
仅术后第3天测量PCT无法预测小儿体外循环心脏直视手术中的感染。PCT与CRP和WBC联合使用可能会增强早期感染预测能力,不过仍需在更大规模的多中心队列中进行进一步验证。