Meuzelaar R R, Schiphorst A H W, Burgmans J P J
Department of Surgery, Diakonessenhuis, Utrecht, The Netherlands.
Department of Surgery, Erasmus Medical Center, Rotterdam, The Netherlands.
Hernia. 2025 May 15;29(1):164. doi: 10.1007/s10029-025-03327-6.
Although the recurrence rate after inguinal hernia repair is low, it remains an important postoperative outcome. To further reduce this rate, modifiable risk factors should be addressed. This study assessed reoperations for recurrence-like complaints following adjustments to the intraoperative protocol aimed at preventing recurrent inguinal hernias. These adjustments included fixating mesh in large unilateral direct defects and large bilateral hernias, and thoroughly reducing inguinal lipomas.
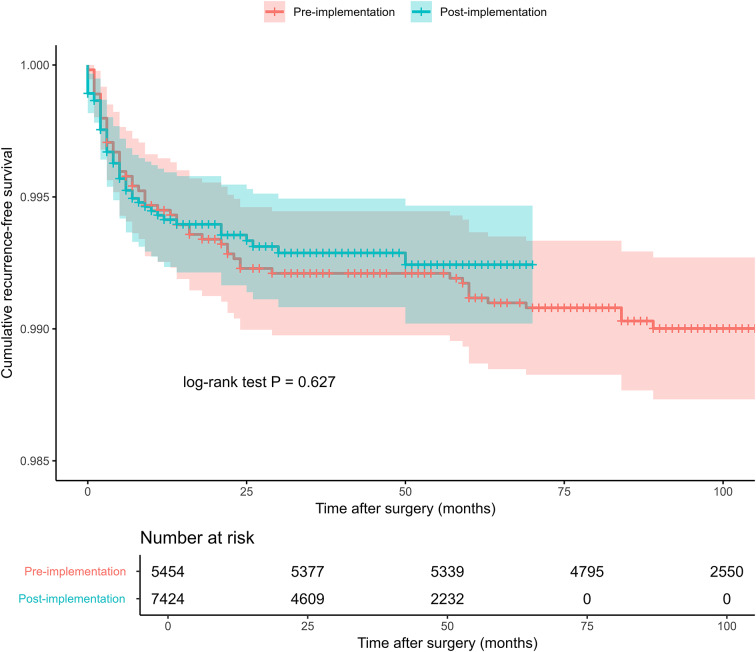
Elective totally extraperitoneal (TEP) repairs in adults performed between January 1, 2013, and October 25, 2023, were retrospectively included. The cohort was subsequently divided into two groups based on the timing of their TEP repair: before (pre-implementation) or after (post-implementation) the protocol adjustments. The primary outcome was reoperation for recurrence-like complaints following the initial TEP repair. Secondary outcomes included mesh fixation and lipoma reduction.
A total of 12,878 TEP repairs in 12,507 patients were included (pre-implementation: 5,454; post-implementation: 7,424). Reoperation rate decreased from 0.97% pre-implementation to 0.65% post-implementation (p = 0.630). Following protocol implementation, mesh fixation for unilateral hernias significantly increased from 3.2% to 5.4% (p < 0.001), and for bilateral hernias from 9.8% to 16.3% (p < 0.001). Lipoma reduction was similar between the groups (unilateral: 32.3-32.6%, p = 0.625; bilateral: 36.0-38.1%, p = 0.288).
The adjusted intraoperative protocol demonstrated a non-significant declining trend of reoperations for recurrence-like complaints. Lipoma reduction was already well-implemented. While mesh fixation increased, it had no significant effect on the recurrence rate, so careful selection of hernias requiring fixation warrants attention.
尽管腹股沟疝修补术后的复发率较低,但它仍是一项重要的术后结果。为了进一步降低这一比率,应解决可改变的风险因素。本研究评估了针对旨在预防复发性腹股沟疝的术中方案进行调整后,因类似复发症状而进行的再次手术情况。这些调整包括在大型单侧直疝缺损和大型双侧疝中固定补片,以及彻底切除腹股沟脂肪瘤。
回顾性纳入2013年1月1日至2023年10月25日期间在成人中进行的择期完全腹膜外(TEP)修补术。随后根据TEP修补的时间将队列分为两组:方案调整前(实施前)或调整后(实施后)。主要结局是初次TEP修补术后因类似复发症状而进行的再次手术。次要结局包括补片固定和脂肪瘤切除。
共纳入12507例患者的12878例TEP修补术(实施前:5454例;实施后:7424例)。再次手术率从实施前的0.97%降至实施后的0.65%(p = 0.630)。方案实施后,单侧疝的补片固定率从3.2%显著增加至5.4%(p < 0.001),双侧疝从9.8%增加至16.3%(p < 0.001)。两组间脂肪瘤切除情况相似(单侧:32.3 - 32.6%,p = 0.625;双侧:36.0 - 38.1%,p = 0.288)。
调整后的术中方案显示,因类似复发症状而进行的再次手术有非显著的下降趋势。脂肪瘤切除已得到很好的实施。虽然补片固定增加了,但对复发率没有显著影响,因此需要谨慎选择需要固定的疝。