Rahman Afruna, Ray Meghna, Madewell Zachary J, Igunza Kitiezo Aggrey, Akelo Victor, Onyango Dickens, Murila Florence, Mwebia Winnie, Ogbuanu Ikechukwu Udo, Ojulong Julius, Kowuor Dickens, Kaluma Erick, Samura Solomon, El Arifeen Shams, Gurley Emily S, Hossain Mohammad Zahid, Islam Kazi Munisul, Biswas Rajib, Assefa Nega, Teferi Temesgen, Eshetu Konjit, Madrid Lola, Kotloff Karen L, Tapia Milagritos D, Keita Adama Mamby, Xerinda Elisio, de Assis Celisa Mendonça, Kincardett Milton, Mandomado Inacio, Varo Rosauro, Madhi Shabir A, Dangor Ziyaad, Baba Vuyelwa, Velaphi Sithembiso, Adam Yasmin, Blau Dianna M, Mutevedzi Portia C, Bassat Quique, Whitney Cynthia G, Rees Chris A
International Centre for Diarrhoeal Disease Research Bangladesh (ICDDRB), Dhaka, Bangladesh.
Hubert Department of Global Health, Rollins School of Public Health, Emory University, Atlanta, Georgia.
JAMA Netw Open. 2025 May 1;8(5):e2510790. doi: 10.1001/jamanetworkopen.2025.10790.
Most of the 2.3 million annual neonatal deaths occur in sub-Saharan Africa and South Asia, with perinatal asphyxia and neonatal sepsis being the leading causes of neonatal mortality. Most neonatal deaths are considered preventable through high-quality clinical care, which includes adherence to clinical care guidelines.
To assess adherence to World Health Organization clinical care guidelines for management of perinatal asphyxia and neonatal sepsis and to identify patient-level factors in adherence among neonates who died from these conditions.
DESIGN, SETTING, AND PARTICIPANTS: This cross-sectional study obtained data from December 2015 through October 2023 from the Child Health and Mortality Prevention Surveillance (CHAMPS) catchment areas in 7 low- and middle-income countries in sub-Saharan Africa (Ethiopia, Kenya, Mali, Mozambique, Sierra Leone, and South Africa) and South Asia (Bangladesh). Participants were neonates who were born alive and were aged 0 to 28 days at the time of death and had either perinatal asphyxia or neonatal sepsis.
Medical records of neonates who died from perinatal asphyxia or neonatal sepsis determined by postmortem diagnostics.
The main outcome was the proportion of deceased neonates who received guideline-adherent treatments before they died. Mixed-effect multivariable logistic regression analyses were performed to identify factors associated with administration of at least bag-valve-mask (BVM) ventilation for perinatal asphyxia.
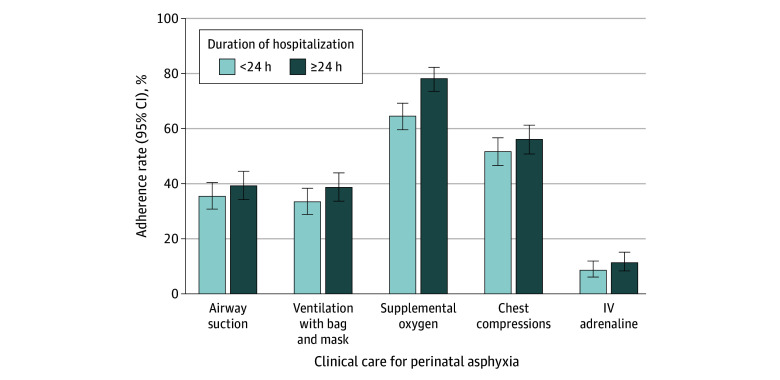
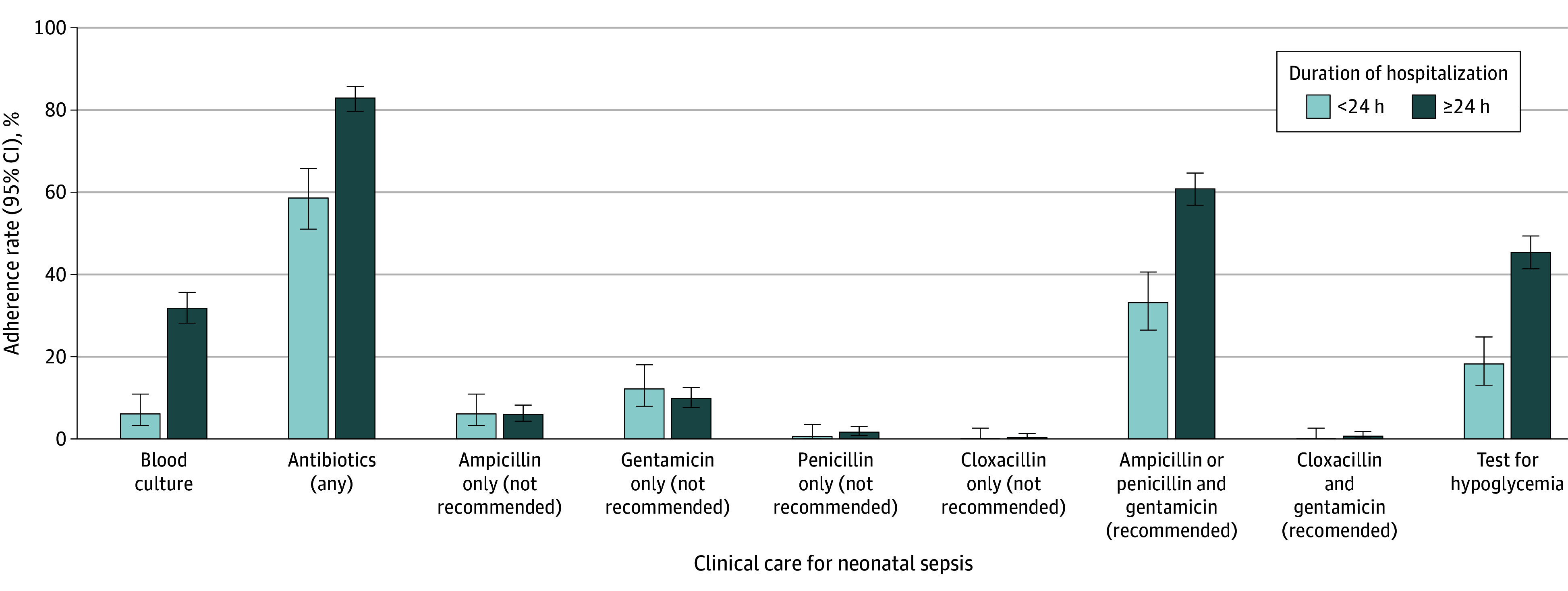
Of the 1194 neonates (median [IQR] age at the time of death, 2 [1-6] days; 692 males [58.0%]) who died and were enrolled in CHAMPS with available clinical data, 476 (39.9%) died from perinatal asphyxia, 562 (47.0%) died from neonatal sepsis, and 156 (13.1%) from both conditions. These neonates had a median (IQR) birth weight of 2130 (1266-2988) g. For cases with perinatal asphyxia, guideline adherence ranged from 12.2% (n = 77) for adrenaline administration to 85.4% (540) for supplemental oxygen administration. Only 4.4% of neonates (28) with perinatal asphyxia received all recommended treatments. Among cases with neonatal sepsis, antibiotics were administered to 86.8% (623), although the recommended treatment was administered to only 61.0% (438). In multivariable analyses, neonates in whom clinicians accurately identified perinatal asphyxia were more likely to receive BVM ventilation than those who had received discordant antemortem and postmortem diagnoses (adjusted odds ratio, 2.00; 95% CI, 1.29-3.12).
In this cross-sectional study, clinical care guideline adherence was suboptimal among neonates who died from perinatal asphyxia or neonatal sepsis. This finding underscores the critical need to increase adherence in regions with high rates of neonatal mortality and may inform strategies for strengthening health systems to support compliance with clinical care guidelines.
每年230万例新生儿死亡中,大多数发生在撒哈拉以南非洲和南亚,围产期窒息和新生儿败血症是新生儿死亡的主要原因。大多数新生儿死亡被认为可通过高质量的临床护理预防,其中包括遵循临床护理指南。
评估对世界卫生组织围产期窒息和新生儿败血症管理临床护理指南的遵循情况,并确定死于这些病症的新生儿中与遵循情况相关的患者层面因素。
设计、地点和参与者:这项横断面研究收集了2015年12月至2023年10月期间来自撒哈拉以南非洲(埃塞俄比亚、肯尼亚、马里、莫桑比克、塞拉利昂和南非)和南亚(孟加拉国)7个低收入和中等收入国家儿童健康与死亡率预防监测(CHAMPS)集水区的数据。参与者为出生时存活、死亡时年龄在0至28天且患有围产期窒息或新生儿败血症的新生儿。
通过尸检诊断确定死于围产期窒息或新生儿败血症的新生儿的医疗记录。
主要结局是死亡前接受指南推荐治疗的死亡新生儿比例。进行混合效应多变量逻辑回归分析,以确定与围产期窒息至少接受袋阀面罩(BVM)通气相关的因素。
在1194例死亡且纳入CHAMPS并有可用临床数据的新生儿中(死亡时年龄中位数[四分位间距]为2[1 - 6]天;692例男性[58.0%]),476例(39.9%)死于围产期窒息,562例(47.0%)死于新生儿败血症,156例(13.1%)死于两种病症。这些新生儿出生体重中位数(四分位间距)为2130(1266 - 2988)g。对于围产期窒息病例,指南遵循率从肾上腺素给药的12.2%(n = 77)到补充氧气给药的85.4%(540)不等。只有4.4%(28例)围产期窒息新生儿接受了所有推荐治疗。在新生儿败血症病例中,86.8%(623例)使用了抗生素,尽管只有61.0%(438例)接受了推荐治疗。在多变量分析中,临床医生准确识别围产期窒息的新生儿比生前和死后诊断不一致的新生儿更有可能接受BVM通气(调整优势比为2.00;95%置信区间为1.29 - 3.12)。
在这项横断面研究中,死于围产期窒息或新生儿败血症的新生儿对临床护理指南的遵循情况不理想。这一发现强调了在新生儿死亡率高的地区提高遵循率的迫切需求,并可能为加强卫生系统以支持遵守临床护理指南的策略提供参考。