Rees Chris A, Igunza Kitiezo Aggrey, Madewell Zachary J, Akelo Victor, Onyango Dickens, El Arifeen Shams, Gurley Emily S, Hossain Mohammad Zahid, Rahman Afruna, Alam Muntasir, Scott J Anthony G, Assefa Nega, Madrid Lola, Belachew Anteneh, Leulseged Haleluya, Kotloff Karen L, Sow Samba O, Tapia Milagritos D, Keita Adama Mamby, Sidibe Diakaridia, Sitoe Antonio, Varo Rosauro, Ajanovic Sara, Bassat Quique, Mandomando Inácio, Tippett Barr Beth A, Ogbuanu Ikechukwu, Cain Carrie Jo, Bassey Ima-Abasi, Luke Ronita, Gassama Khadija, Madhi Shabir, Dangor Ziyaad, Mahtab Sana, Velaphi Sithembiso, du Toit Jeanie, Mutevedzi Portia C, Blau Dianna M, Breiman Robert F, Whitney Cynthia G
Department of Pediatrics, Emory University School of Medicine, Atlanta, GA, United States of America.
Children's Healthcare of Atlanta, Atlanta, GA, United States of America.
EClinicalMedicine. 2023 Aug 31;63:102198. doi: 10.1016/j.eclinm.2023.102198. eCollection 2023 Sep.
Most childhood deaths globally are considered preventable through high-quality clinical care, which includes adherence to clinical care recommendations. Our objective was to describe adherence to World Health Organization recommendations for the management of leading causes of death among children.
We conducted a retrospective, descriptive study examining clinical data for children aged 1-59 months who were hospitalized and died in a Child Health and Mortality Prevention Surveillance (CHAMPS) catchment, December 2016-June 2021. Catchment areas included: Baliakandi and Faridpur, Bangladesh; Kersa, Haramaya, and Harar, Ethiopia; Kisumu and Siaya, Kenya; Bamako, Mali; Manhiça and Quelimane, Mozambique; Makeni, Sierra Leone; Soweto, South Africa. We reviewed medical records of those who died from lower respiratory tract infections, sepsis, malnutrition, malaria, and diarrheal diseases to determine the proportion who received recommended treatments and compared adherence by hospitalization duration.
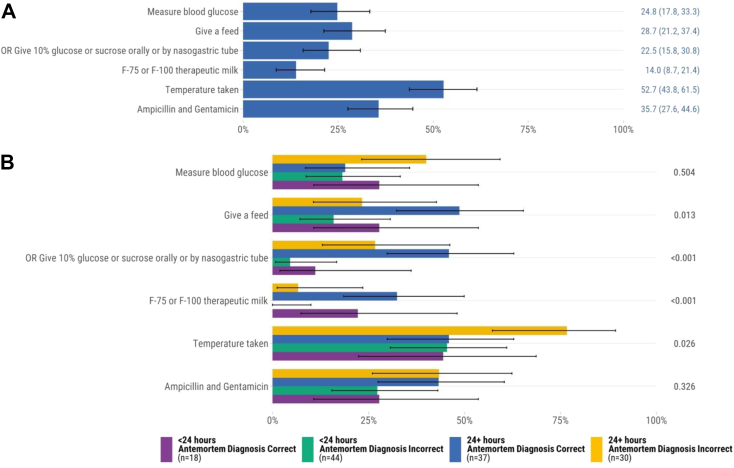
CHAMPS enrolled 460 hospitalized children who died from the leading causes (median age 12 months, 53.0% male). Median hospital admission was 31 h. There were 51.0% (n = 127/249) of children who died from lower respiratory tract infections received supplemental oxygen. Administration of intravenous fluids for sepsis (15.9%, n = 36/226) and supplemental feeds for malnutrition (14.0%, n = 18/129) were uncommon. There were 51.4% (n = 55/107) of those who died from malaria received antimalarials. Of the 80 children who died from diarrheal diseases, 76.2% received intravenous fluids. Those admitted for ≥24 h more commonly received antibiotics for lower respiratory tract infections and sepsis, supplemental feeds for malnutrition, and intravenous fluids for sepsis than those admitted <24 h.
Provision of recommended clinical care for leading causes of death among young children was suboptimal. Further studies are needed to understand the reasons for deficits in clinical care recommendation adherence.
Bill & Melinda Gates Foundation.
全球大多数儿童死亡被认为可通过高质量的临床护理预防,其中包括遵循临床护理建议。我们的目标是描述对世界卫生组织关于儿童主要死因管理建议的遵循情况。
我们开展了一项回顾性描述性研究,审查2016年12月至2021年6月在儿童健康与死亡率预防监测(CHAMPS)覆盖地区住院并死亡的1至59个月儿童的临床数据。覆盖地区包括:孟加拉国的巴利亚坎迪和法里德布尔;埃塞俄比亚的克尔萨、哈拉马亚和哈勒尔;肯尼亚的基苏木和锡亚;马里的巴马科;莫桑比克的马尼亚卡和克利马内;塞拉利昂的马克尼;南非的索韦托。我们审查了因下呼吸道感染、败血症、营养不良、疟疾和腹泻病死亡者的病历,以确定接受推荐治疗的比例,并比较按住院时间的遵循情况。
CHAMPS登记了460名因主要死因住院死亡的儿童(中位年龄12个月,53.0%为男性)。中位住院时间为31小时。因下呼吸道感染死亡的儿童中有51.0%(n = 127/249)接受了补充氧气治疗。因败血症使用静脉输液(15.9%,n = 36/226)和因营养不良提供补充喂养(14.0%,n = 18/129)的情况并不常见。因疟疾死亡的儿童中有51.4%(n = 55/107)接受了抗疟药治疗。在80名因腹泻病死亡的儿童中,76.2%接受了静脉输液。住院≥24小时的儿童比住院<24小时的儿童更常因下呼吸道感染和败血症接受抗生素治疗、因营养不良接受补充喂养以及因败血症接受静脉输液。
为幼儿主要死因提供推荐临床护理的情况并不理想。需要进一步研究以了解临床护理建议遵循不足的原因。
比尔及梅琳达·盖茨基金会。