Liu Song, Yang Tianhao, Wei Ming, Wang Huiying, Ren Tao, Cao Chen, Sun Yu, Fu Lejun, Hao Nina, Wang Sifei, Luo Leilei, Wang Luotong, Xia Shuang, Jin Song, Tian Chao
Department of Radiology, Tianjin Huanhu Hospital, Tianjin, China.
Department of Neurosurgery, Tianjin Huanhu Hospital, Tianjin, China.
Quant Imaging Med Surg. 2025 May 1;15(5):4085-4100. doi: 10.21037/qims-24-1073. Epub 2025 Apr 28.
A comprehensive assessment of collateral status can yield profound insights into the ischemic mechanism in patients experiencing acute ischemic stroke. This study aims to investigate whether time-variant and tissue-level collateral characteristics may serve as predictors for functional outcomes in patients undergoing endovascular thrombectomy (EVT) through the application of machine learning (ML) algorithms, and to stratify postoperative neurological recovery of these patients.
In this retrospective study, 128 acute ischemic stroke patients characterized by anterior large-vessel occlusion and received EVT between May 2020 and December 2022 were enrolled. These patients underwent multiphase computed tomography (CT) angiography (mCTA) and CT perfusion (CTP). The time-variant collateral score was defined as the Collateral Score on Color-Coded summation maps (CSCC) of mCTA. The hypoperfusion intensity ratio (HIR) was calculated from CTP data. The data were split into training and test sets in a ratio of 7:3, and univariable and multivariable regression analyses were employed for feature selection. For ML analyses, logistic regression (LR), support vector machine (SVM), random forest (RF), decision tree (DT), and eXtreme gradient boosting (XGBoost) algorithms were utilized. The receiver operating characteristic (ROC) curve and decision curve were employed for performance evaluation. The mixed effect model was established to estimate the impact of collateral stratification on the postoperative National Institutes of Health Stroke Scale (NIHSS).
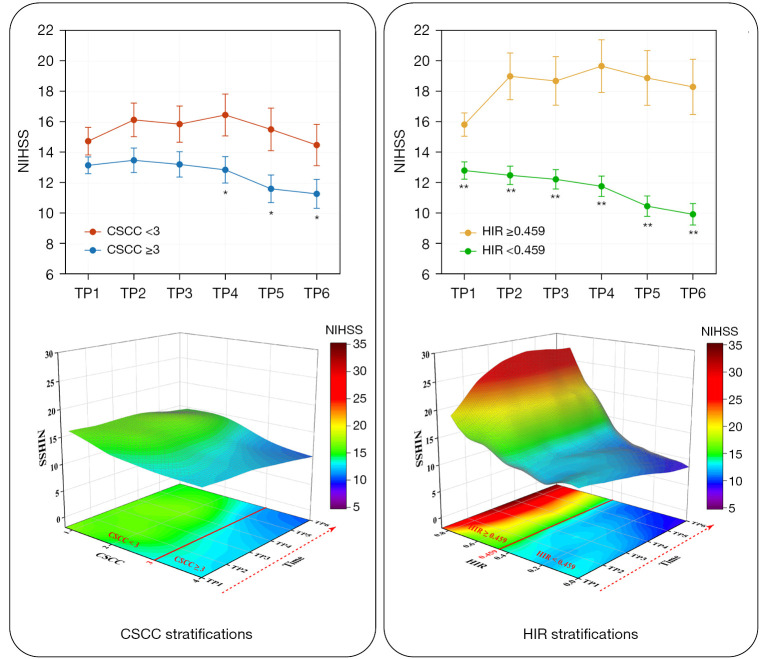
Age [odds ratio (OR) =1.073; 95% confidence interval (CI): 1.008, 1.154; P=0.040], Alberta Stroke Program Early CT Score (ASPECTS) (OR =0.742; 95% CI: 0.546, 0.975; P=0.040), CSCC (OR =0.468; 95% CI: 0.213, 0.953; P=0.044), and HIR (OR =56.666; 95% CI: 3.843, 1,156.959; P=0.005) were significantly associated with good outcome in training set. By utilizing these four selected features, the RF algorithm achieved the best performance and the highest clinical suitability in predicting good clinical outcomes, with an area under the ROC curve (AUC) of 0.964 (95% CI: 0.902, 0.992) and 0.837 (95% CI: 0.684, 0.935) in training set and testing set, respectively. The Shapley Additive exPlanations (SHAP) analysis revealed that HIR was the most significant variable in predicting clinical outcomes. Fixed effects and group × time interaction effects [all P<0.01 at all time points (TPs)] were acquired in HIR stratification. HIR enabled better stratification and prediction of patients' postoperative NIHSS [Akaike information criterion (AIC): HIR =4,599.577 and CSCC =4,648.707].
RF model, which has been trained on time-variant and tissue-level collaterals, is capable of accurately predicting the clinical outcomes of patients undergoing EVT. Stratifying patients based on HIR may yield valuable insights into predicting trends in the potential postoperative neurological recovery.
对侧支循环状态进行全面评估能够深入洞察急性缺血性脑卒中患者的缺血机制。本研究旨在通过应用机器学习(ML)算法,探讨时变和组织水平的侧支循环特征是否可作为接受血管内血栓切除术(EVT)患者功能结局的预测指标,并对这些患者术后的神经功能恢复进行分层。
在这项回顾性研究中,纳入了128例2020年5月至2022年12月期间以大脑前大血管闭塞为特征并接受EVT的急性缺血性脑卒中患者。这些患者接受了多期计算机断层扫描(CT)血管造影(mCTA)和CT灌注(CTP)检查。时变侧支循环评分定义为mCTA彩色编码求和图上的侧支循环评分(CSCC)。从CTP数据计算低灌注强度比(HIR)。数据按7:3的比例分为训练集和测试集,并采用单变量和多变量回归分析进行特征选择。对于ML分析,使用了逻辑回归(LR)、支持向量机(SVM)、随机森林(RF)、决策树(DT)和极端梯度提升(XGBoost)算法。采用受试者工作特征(ROC)曲线和决策曲线进行性能评估。建立混合效应模型以估计侧支循环分层对术后美国国立卫生研究院卒中量表(NIHSS)的影响。
在训练集中,年龄[比值比(OR)=1.073;95%置信区间(CI):1.008,1.154;P = 0.040]、阿尔伯塔卒中项目早期CT评分(ASPECTS)(OR = 0.742;95%CI:0.546,0.975;P = 0.040)、CSCC(OR = 0.468;95%CI:0.213,0.953;P = 0.044)和HIR(OR = 56.666;95%CI:3.843,1156.959;P = 0.005)与良好结局显著相关。利用这四个选定特征,RF算法在预测良好临床结局方面表现最佳且临床适用性最高,训练集和测试集的ROC曲线下面积(AUC)分别为0.964(95%CI:0.902,0.992)和0.837(95%CI:0.684,0.935)。Shapley加性解释(SHAP)分析表明,HIR是预测临床结局中最显著的变量。在HIR分层中获得了固定效应和组×时间交互效应[所有时间点(TPs)的P均<0.01]。HIR能够更好地对患者术后NIHSS进行分层和预测[赤池信息准则(AIC):HIR = 4599.577,CSCC = 4648.707]。
基于时变和组织水平侧支循环训练的RF模型能够准确预测接受EVT患者的临床结局。基于HIR对患者进行分层可能为预测潜在术后神经功能恢复趋势提供有价值的见解。