Christou Georgios A, Letsas Konstantinos P, Konstandi Maria, Christou Maria A, Christou Konstantinos A, Kyriakopoulos Christos, Vidalakis Eleftherios, Tigas Stelios, Christodoulou Dimitrios K, Kiortsis Dimitrios N
Department of Radiology, Faculty of Medicine, University of Ioannina, Ioannina, Greece.
Atherothrombosis Research Centre, Faculty of Medicine, University of Ioannina, Ioannina, Greece.
Front Cardiovasc Med. 2025 May 2;12:1537078. doi: 10.3389/fcvm.2025.1537078. eCollection 2025.
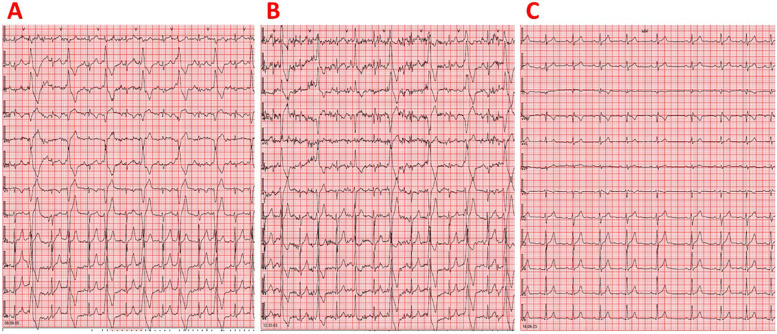
The detection of frequent premature ventricular contractions (PVCs) in an athlete represents one of the most important red flags during pre-participation screening. We report the case of a 6-year-old asymptomatic male athlete practicing basketball and sailing, who was examined for pre-participation screening. His resting electrocardiogram showed very frequent, isolated, monomorphic PVCs. The PVCs exhibited a left bundle branch block morphology with an inferior axis and R/S wave precordial transition in lead V3. The most likely origin of PVCs was considered the left ventricular outflow tract. Resting transthoracic echocardiography revealed reduced left ventricular systolic function, with an ejection fraction of 43%, indicating the possible existence of PVC-induced cardiomyopathy. We detected 43,149 isolated monomorphic PVCs (PVC burden: 40%) on 24-h ambulatory electrocardiographic monitoring. Initiation of treatment with atenolol 12.5 mg twice a day led to inadequate reduction of PVCs, with 29,452 isolated monomorphic PVCs (PVC burden: 29%) still observed on 24-h ambulatory electrocardiographic monitoring. After adding flecainide 25 mg twice daily to atenolol treatment, 24-h ambulatory electrocardiographic monitoring revealed complete resolution of ventricular arrhythmias, with no PVCs detected. Left ventricular systolic function recovered to normal. At 12 years of age, the athlete remained on combination therapy with atenolol and flecainide, continued participating in sports, and remained completely asymptomatic with normal cardiac examinations. The optimization of drug treatment was favored over catheter ablation since the athlete was a child and the probable origin of PVCs was the left ventricular outflow tract. This case report highlights that flecainide at a relatively low dose as an add-on therapy to a beta-blocker was highly effective and safe for treating high-burden PVCs originating from the ventricular outflow tract in a juvenile athlete.
运动员中频繁室性早搏(PVC)的检测是参与运动前筛查时最重要的警示信号之一。我们报告一例6岁无症状男性运动员的病例,该运动员从事篮球和帆船运动,接受了运动前筛查。他的静息心电图显示非常频繁、孤立、单形性PVC。这些PVC表现为左束支传导阻滞形态,电轴向下,V3导联R/S波胸前导联移行。PVC最可能的起源被认为是左心室流出道。静息经胸超声心动图显示左心室收缩功能降低,射血分数为43%,提示可能存在PVC诱发的心肌病。在24小时动态心电图监测中,我们检测到43149次孤立单形性PVC(PVC负荷:40%)。开始每天两次服用12.5mg阿替洛尔治疗后,PVC减少不充分,24小时动态心电图监测仍观察到29452次孤立单形性PVC(PVC负荷:29%)。在阿替洛尔治疗中加用每日两次25mg氟卡尼后,24小时动态心电图监测显示室性心律失常完全消失,未检测到PVC。左心室收缩功能恢复正常。在12岁时,该运动员继续接受阿替洛尔和氟卡尼联合治疗,继续参加运动,心脏检查正常且完全无症状。由于该运动员是儿童且PVC可能起源于左心室流出道,因此药物治疗优化优于导管消融。本病例报告强调,相对低剂量的氟卡尼作为β受体阻滞剂的附加疗法,对于治疗青少年运动员源于心室流出道的高负荷PVC非常有效且安全。