Zhang Hui, Li Yueyun, Liu Yuhang, Li Haonan, Wang Hong
School of Medical Business, Guangdong Pharmaceutical University, Guangzhou, Guangdong, China.
Guangdong Health Economics and Promotion Research Center, Guangdong Pharmaceutical University, Guangzhou, Guangdong, China.
Front Pharmacol. 2025 May 2;16:1527614. doi: 10.3389/fphar.2025.1527614. eCollection 2025.
The combination of amivantamab and lazertinib has demonstrated clinically significant and sustained antitumor effects in both treatment-naïve and osimertinib-pretreated advanced non-small cell lung cancer (NSCLC) patients harboring previously untreated epidermal growth factor receptor (EGFR) mutations.
A cost-effectiveness analysis was conducted to compare three therapeutic strategies, namely, amivantamab with lazertinib combination therapy, lazertinib monotherapy, and osimertinib monotherapy, for advanced NSCLC patients with EGFR mutations; the patients included both treatment-naïve individuals and those previously treated with osimertinib.
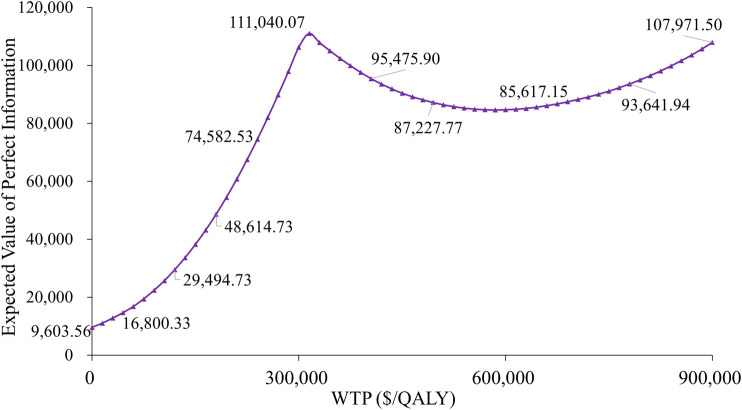
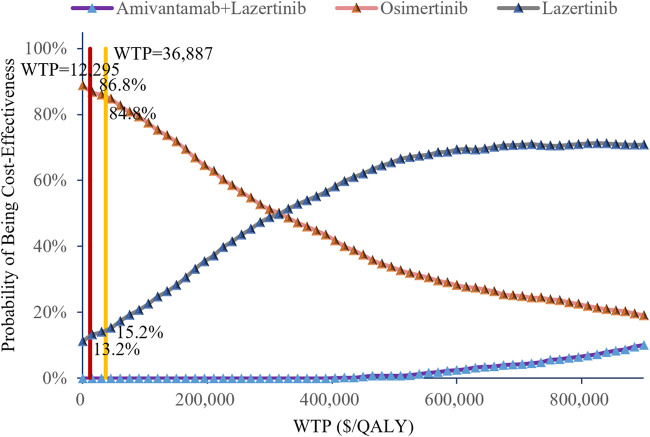
Based on a previous multicenter randomized double-blind phase III trial (NCT04487080) for evaluating amivantamab-lazertinib versus osimertinib in EGFR-mutated advanced NSCLC patients (both treatment-naïve and osimertinib-pretreated), we constructed a Markov model for 3-week cycles over a 5-year horizon. The primary outcomes of the model included total costs, quality-adjusted life years (QALYs), and incremental cost-effectiveness ratio (ICER), where all economic parameters were discounted at 3.0% annually. The cost-utility analyses employed China's gross domestic product for 2023 (ranging from $12,295.7 to $36,887.0) as the willingness-to-pay (WTP) threshold supplemented by comprehensive sensitivity and scenario analyses to verify the model robustness.
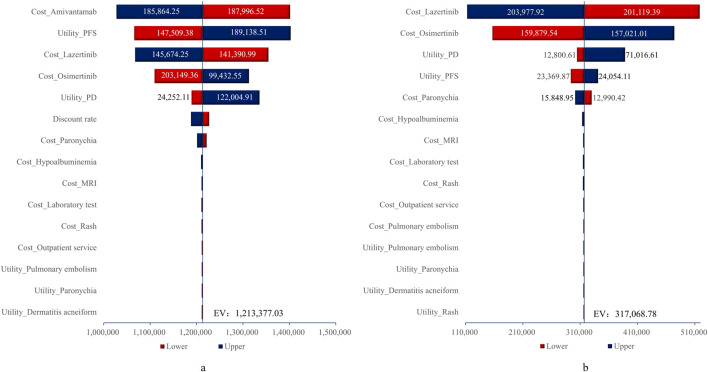
The economic evaluations demonstrated that compared to osimertinib monotherapy, the amivantamab-lazertinib combination yielded an additional 1.11 QALYs at an incremental cost of $1,342,374, producing an ICER of $1,211,236/QALY that substantially exceeds the $36,887 WTP threshold. Similarly, lazertinib monotherapy showed a QALY gain of 0.71 with $224,248 of additional costs (ICER = $315,640/QALY), also surpassing the lower threshold of $12,296. The sensitivity analysis showed that the predominant model driver was drug acquisition costs.
The economic analyses indicate that neither amivantamab-lazertinib combination therapy nor lazertinib monotherapy represents a cost-effective first-line option for EGFR exon 20 insertion-positive NSCLC compared to osimertinib monotherapy. The substantial drug acquisition costs are the primary contributors to the unfavorable economic profiles of these treatments. Hence, future clinical implementations should carefully weigh the considerable therapeutic benefits against the significant financial burdens to achieve an optimal risk-benefit equilibrium.
在既往未接受过治疗以及接受过奥希替尼治疗的、携带此前未治疗过的表皮生长因子受体(EGFR)突变的晚期非小细胞肺癌(NSCLC)患者中,阿米万他单抗与拉泽替尼联合用药已显示出具有临床意义的持续抗肿瘤效果。
进行一项成本效益分析,以比较三种治疗策略,即阿米万他单抗与拉泽替尼联合治疗、拉泽替尼单药治疗以及奥希替尼单药治疗,用于EGFR突变的晚期NSCLC患者;这些患者包括既往未接受过治疗的个体以及既往接受过奥希替尼治疗的个体。
基于之前一项多中心随机双盲III期试验(NCT04487080),该试验评估了阿米万他单抗-拉泽替尼与奥希替尼在EGFR突变的晚期NSCLC患者(既往未接受过治疗以及接受过奥希替尼治疗)中的疗效,我们构建了一个马尔可夫模型,为期5年,周期为3周。该模型的主要结局包括总成本、质量调整生命年(QALY)以及增量成本效益比(ICER),所有经济参数均按每年3.0%进行贴现。成本效用分析采用中国2023年的国内生产总值(范围为12,295.7美元至36,887.0美元)作为支付意愿(WTP)阈值,并辅以全面的敏感性和情景分析以验证模型的稳健性。
经济评估表明,与奥希替尼单药治疗相比,阿米万他单抗-拉泽替尼联合治疗额外产生1.11个QALY,增量成本为1,342,374美元,ICER为1,211,236美元/QALY,大大超过了36,887美元的WTP阈值。同样,拉泽替尼单药治疗显示QALY增加0.71,额外成本为224,248美元(ICER = 315,640美元/QALY),也超过了12,296美元的较低阈值。敏感性分析表明,模型的主要驱动因素是药品采购成本。
经济分析表明,与奥希替尼单药治疗相比,阿米万他单抗-拉泽替尼联合治疗和拉泽替尼单药治疗都不是EGFR外显子20插入阳性NSCLC具有成本效益的一线选择。高昂的药品采购成本是这些治疗方案经济状况不佳的主要原因。因此,未来的临床应用应仔细权衡可观的治疗益处与巨大的经济负担,以实现最佳的风险效益平衡。