Lebel Asaf, Chanchlani Rahul, Cockovski Vedran, Dart Allison, Fleming Adam James, Garg Amit X, Jeyakumar Nivethika, Kim Kirby, Kitchlu Abhijat, McArthur Eric, Nash Danielle, Nathan Paul C, Parekh Rulan S, Pearl Rachel, Pole Jason, Ramphal Raveena, Reid Jennifer, Schechter-Finkelstein Tal, Sung Lillian, Wald Ron, Wang Stella, Wong Peter, Zappitelli Michael
Division of Nephrology, Department of Paediatrics, The Hospital for Sick Children, Toronto, Ontario, Canada.
Pediatric Nephrology Unit, Ha'Emek Medical Center, Afula, Israel.
JAMA Netw Open. 2025 May 1;8(5):e258199. doi: 10.1001/jamanetworkopen.2025.8199.
Post-cancer therapy kidney outcomes, including chronic kidney disease (CKD) and hypertension, are common in childhood cancer survivors (CCS). The incidence and timing of CKD and hypertension in CCS compared with other at-risk or general populations are unclear.
To determine the association of childhood cancer treatment with post-cancer therapy CKD or hypertension.
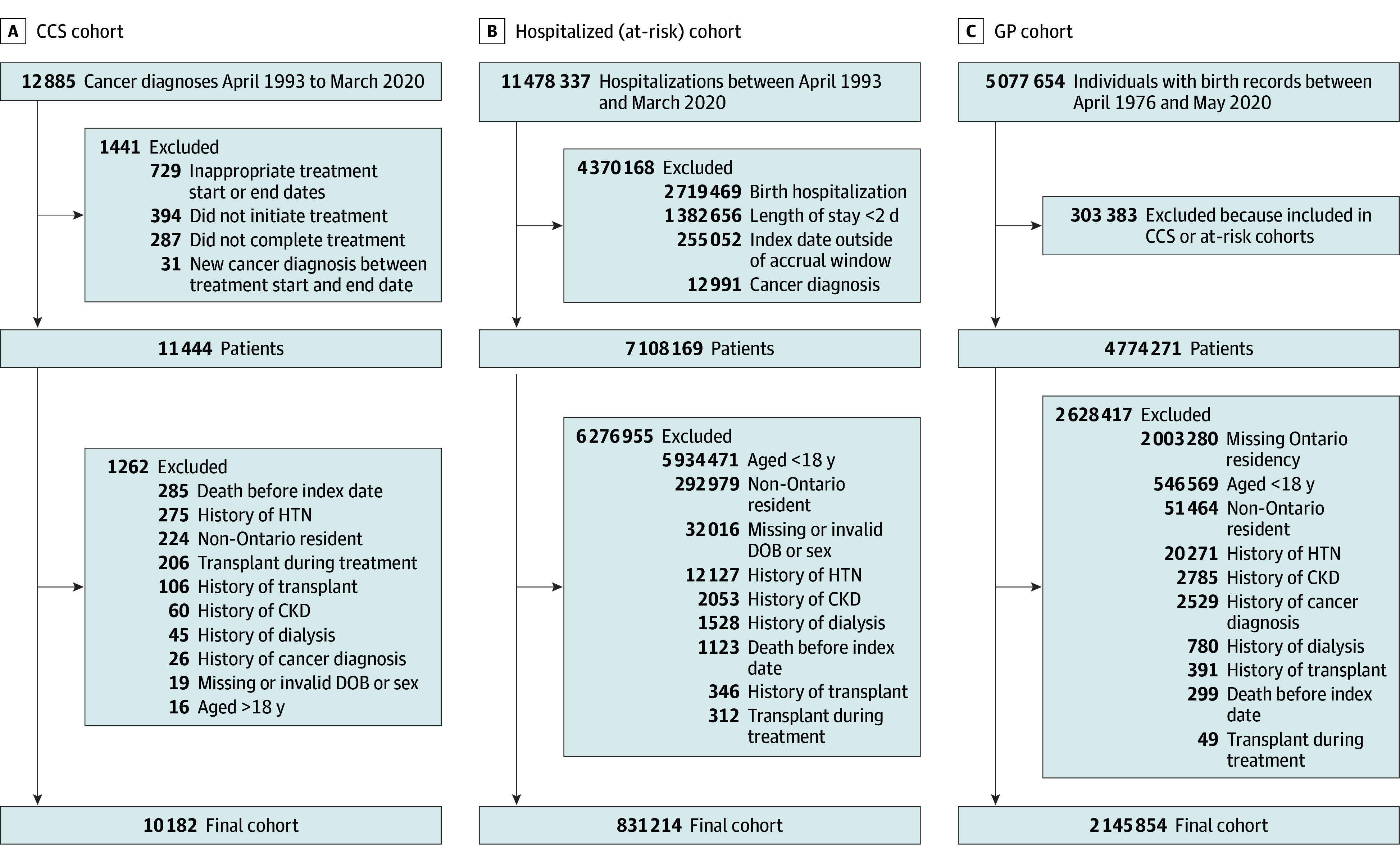
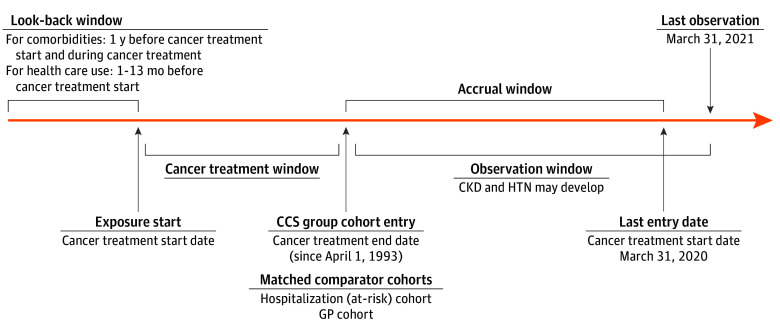
DESIGN, SETTING, AND PARTICIPANTS: Population-based matched cohort study of children treated for cancer between April 1993 and March 2020 in Ontario, Canada, with follow-up until March 2021. The CCS (exposed) cohort included children (≤18 years) surviving cancer. Comparator cohorts were a hospitalization cohort (children who were hospitalized) and a general pediatric population (GP) cohort (all other Ontario children). Exclusion criteria were history of previous cancer, organ transplant, CKD, dialysis, or hypertension. Matching with each of the 2 comparator cohorts was performed separately and in a 1:4 ratio by age, sex, rural vs urban status, income quintile, index year, and presence of previous hospitalization. Data were analyzed from March 2021 to August 2024.
Treatment for cancer.
The primary outcome was the composite of CKD or hypertension, defined by administrative health care diagnosis and procedure codes. Fine and Gray subdistribution hazard modeling, accounting for competing risks (death and new cancer diagnosis or relapse) and adjusting for cardiac disease, liver disease, and diabetes, was used to determine the association of cancer treatment with outcomes.
There were 10 182 CCS (median [IQR] age at diagnosis, 7 [3-13] years; 5529 male [54.3%]; median [IQR] follow-up time, 8 [2-15] years) matched to 40 728 hospitalization cohort patients (median [IQR] age at diagnosis, 7 [2-12] years; 5529 male [weighted percentage, 54.3%]; median [IQR] follow-up time, 11 [6-18] years) and 8849 CCS (median [IQR] age at diagnosis, 5 [2-11] years; 4825 male [54.5%]; median [IQR] follow-up time, 7 [2-14] years) matched to 35 307 GP cohort individuals (median [IQR] age at diagnosis, 6 [2-11] years; 4825 male [weighted percentage, 54.5%]; median [IQR] follow-up time, 10 [5-16] years). Most frequent cancer types were leukemia (2948 patients [29.0%]), central nervous system neoplasms (2123 patients [20.9%]), and lymphoma (1583 patients [15.5%]). During observation, cumulative incidence of CKD or hypertension was 20.85% (95% CI, 18.75%-23.02%) in the CCS cohort vs 16.47% (95% CI, 15.21%-17.77%) in the hospitalization cohort and 19.24% (95% CI, 15.99%-22.73%) in the CCS cohort vs 8.05% (95% CI, 6.76%-9.49%) in the GP cohort. CCS were at increased risk of CKD or hypertension compared with the hospitalization cohort (adjusted hazard ratio, 2.00; 95% CI, 1.86-2.14; P < .001) and the GP cohort (adjusted hazard ratio, 4.71; 95% CI, 4.27-5.19; P < .001).
In this population-based study, CCS were at increased risk for CKD and hypertension, which are associated with mortality, suggesting that early detection and treatment of these conditions in CCS may decrease late complications and mortality.
癌症治疗后的肾脏结局,包括慢性肾脏病(CKD)和高血压,在儿童癌症幸存者(CCS)中很常见。与其他高危或普通人群相比,CCS中CKD和高血压的发病率及发生时间尚不清楚。
确定儿童癌症治疗与癌症治疗后CKD或高血压之间的关联。
设计、地点和参与者:基于人群的匹配队列研究,研究对象为1993年4月至2020年3月在加拿大安大略省接受癌症治疗的儿童,随访至2021年3月。CCS(暴露)队列包括癌症存活儿童(≤18岁)。对照队列是住院队列(住院儿童)和普通儿科人群(GP)队列(安大略省的所有其他儿童)。排除标准为既往癌症、器官移植、CKD、透析或高血压病史。与2个对照队列分别按1:4的比例进行匹配,匹配因素包括年龄、性别、城乡状况、收入五分位数、索引年份和既往住院情况。数据于2021年3月至2024年8月进行分析。
癌症治疗。
主要结局是CKD或高血压的复合结局,由行政医疗保健诊断和程序编码定义。采用考虑竞争风险(死亡和新发癌症诊断或复发)并对心脏病、肝病和糖尿病进行校正的Fine和Gray亚分布风险模型,以确定癌症治疗与结局之间的关联。
10182名CCS(诊断时中位[IQR]年龄,7[3 - 13]岁;5529名男性[54.3%];中位[IQR]随访时间,8[2 - 15]年)与40728名住院队列患者(诊断时中位[IQR]年龄,7[2 - 12]岁;5529名男性[加权百分比,54.3%];中位[IQR]随访时间,11[6 - 18]年)匹配,8849名CCS(诊断时中位[IQR]年龄,5[2 - 11]岁;4825名男性[54.5%];中位[IQR]随访时间,7[2 - 14]年)与35307名GP队列个体(诊断时中位[IQR]年龄,6[2 - 11]岁;4825名男性[加权百分比,54.5%];中位[IQR]随访时间,10[5 - 16]年)匹配。最常见的癌症类型为白血病(2948例患者[29.0%])、中枢神经系统肿瘤(2123例患者[20.9%])和淋巴瘤(1583例患者[15.5%])。在观察期间,CCS队列中CKD或高血压的累积发病率为20.85%(95%CI,18.75% - 23.02%),住院队列中为16.47%(95%CI,15.21% - 17.77%),CCS队列与GP队列相比,前者为19.24%(95%CI,15.99% - 22.73%),后者为8.05%(95%CI,6.76% - 9.49%)。与住院队列相比,CCS发生CKD或高血压的风险增加(校正风险比,2.00;95%CI,1.86 - 2.14;P <.001),与GP队列相比风险也增加(校正风险比,4.71;95%CI,4.27 - 5.19;P <.001)。
在这项基于人群的研究中,CCS发生CKD和高血压的风险增加,而这两种疾病与死亡率相关,提示在CCS中早期发现和治疗这些疾病可能会降低晚期并发症和死亡率。