Lawrence Neil R, Dawson Jeremy, Lang Zi-Qiang, Prete Alessandro, Baranowski Elizabeth S, Schiffer Lina, Taylor Angela E, Brac de la Perrière Aude, Hirschberg Angelica Lindén, Juul Anders, Merke Deborah P, Newell-Price John, Rees D Aled, Reisch Nicole, Stikkelbroeck Nike, Touraine Philippe A, Krone Nils, Keevil Brian, Collins Gary S, Arlt Wiebke, Ross Richard J M
School of Medicine and Population Health, University of Sheffield, Sheffield, United Kingdom.
School of Electrical and Electronic Engineering, University of Sheffield, Sheffield, United Kingdom.
EBioMedicine. 2025 Jun;116:105749. doi: 10.1016/j.ebiom.2025.105749. Epub 2025 May 20.
There is no consensus on how to monitor adrenal androgens in Congenital Adrenal Hyperplasia (CAH).
Modelling of serum and salivary steroid profiles in healthy participants and patients with CAH randomised to either standard treatment or modified-release hydrocortisone hard capsules (MRHC).
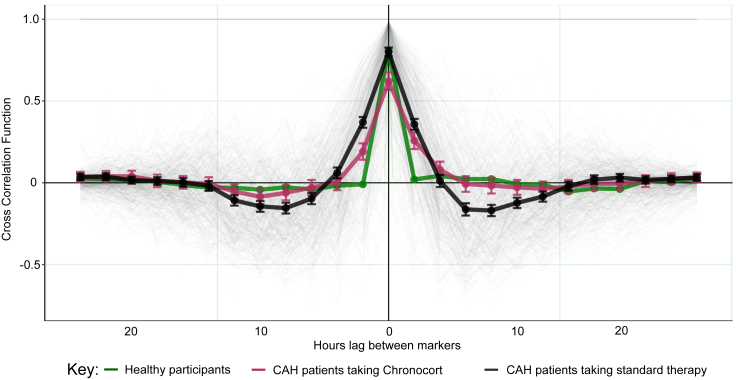
Changes in serum 17-hydroxyprogesterone (17OHP) and androstenedione (A4) paralleled each other in healthy participants (n = 19) and patients with CAH (n = 122). However, healthy participants had similar absolute levels of 17OHP and A4 whereas patients with CAH had proportionally higher levels of 17OHP. Cross-correlation showed no lag between serum 17OHP and A4. In CAH, Bayesian multiple change point analysis converged on a 17OHP of 4.5 nmol/l below which in proportion to 17OHP the A4 is lower. Patients on standard treatment had a morning peak in 17OHP and A4 whereas patients on MRHC had relatively flat profiles. Salivary androgens including 11-ketotestosterone correlated with serum 17OHP and A4 in female patients (r = 0.7 to 0.9).
In CAH, elevated 17OHP drives the production of A4. High A4 reflects poor control, but low A4 does not indicate overtreatment. Accepting 17OHP is higher than A4, both measurements give similar reflection of control, and a 17OHP <38 nmol/l (1250 ng/dl) was associated with an A4 in the normal range <5 nmol/l (143 ng/dl) in 95% of patients and in clinical trials was used to define good control. On MRHC, which controls androgen levels over 24 h, a single sample of 17OHP and/or A4 can be used to monitor control. Salivary measurements reflect similar results to serum.
Diurnal; MRC; NIH; NIHR.
关于如何监测先天性肾上腺皮质增生症(CAH)患者的肾上腺雄激素水平,目前尚无共识。
对健康参与者以及随机接受标准治疗或缓释氢化可的松硬胶囊(MRHC)治疗的CAH患者的血清和唾液类固醇谱进行建模。
在健康参与者(n = 19)和CAH患者(n = 122)中,血清17-羟孕酮(17OHP)和雄烯二酮(A4)的变化相互平行。然而,健康参与者的17OHP和A4绝对水平相似,而CAH患者的17OHP水平相对较高。互相关分析显示血清17OHP和A4之间无滞后现象。在CAH中,贝叶斯多重变化点分析得出17OHP为4.5 nmol/l,低于该值时,A4与17OHP成比例降低。接受标准治疗的患者17OHP和A4在早晨出现峰值,而接受MRHC治疗的患者其水平相对平稳。女性患者的唾液雄激素(包括11-酮睾酮)与血清17OHP和A4相关(r = 0.7至0.9)。
在CAH中,17OHP升高驱动A4的产生。高A4反映控制不佳,但低A4并不表明治疗过度。由于17OHP高于A4,两者的测量结果对疾病控制情况的反映相似,95%的患者17OHP<38 nmol/l(1250 ng/dl)时,A4处于正常范围<5 nmol/l(143 ng/dl),在临床试验中该值被用于定义良好控制。对于能在24小时内控制雄激素水平的MRHC,单次17OHP和/或A4样本即可用于监测疾病控制情况。唾液测量结果与血清测量结果相似。
昼夜节律研究;医学研究委员会;美国国立卫生研究院;英国国家卫生研究院。