Bacchetta Matthew, Bermudez Christian A, Bharat Ankit, Brown A Whitney, Budev Marie M, Cypel Marcelo, Demarest Caitlin T, Dilling Daniel F, Griffith Bartley P, Haney John C, Keshavjee Shaf, Kon Zachary N, Machuca Tiago N, Mallea Jorge M, Pham Si M, Waddell Thomas K, Whitson Bryan A, McCurry Kenneth R
Department of Cardiac Surgery, Vanderbilt University Medical Center, Nashville, TN, USA.
Division of Cardiovascular Surgery, Department of Surgery, University of Pennsylvania, Philadelphia, PA, USA.
J Thorac Dis. 2025 Apr 30;17(4):1832-1843. doi: 10.21037/jtd-2024-2069. Epub 2025 Apr 27.
Ex vivo lung perfusion (EVLP) of donor lungs not otherwise acceptable for transplantation can provide outcomes similar to standard-criteria lung transplantation and has been reported to increase transplant volume by approximately 20% in some transplant centers. Evidence to support decisions about use of EVLP is limited, so expert opinion can be a useful decision aid. This study developed expert consensus recommendations for EVLP with acellular perfusate using a modified Delphi method.
A panel of 18 physicians with expertise in lung transplantation and EVLP who practice in North America completed three surveys on EVLP: Survey 1 used open-ended questions; Survey 2 used primarily Likert-scale questions; and Survey 3 repeated Survey 2 while providing panelists with the Survey 2 results. A follow-up meeting after Survey 3 probed open questions.
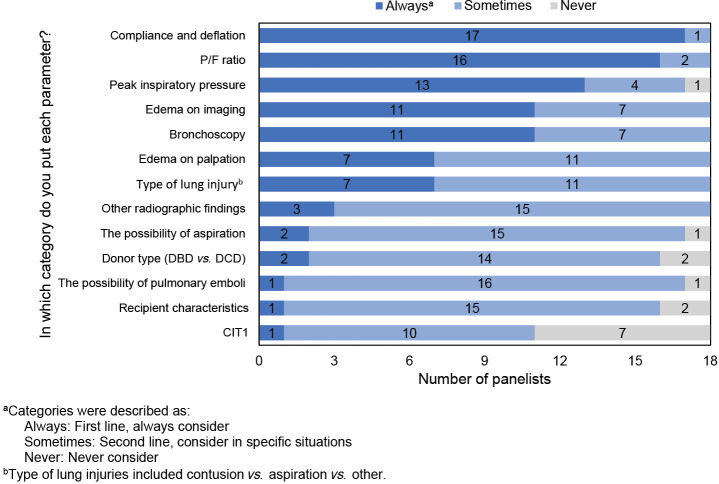
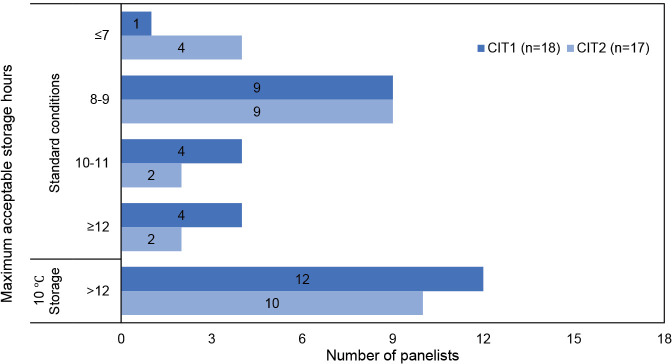
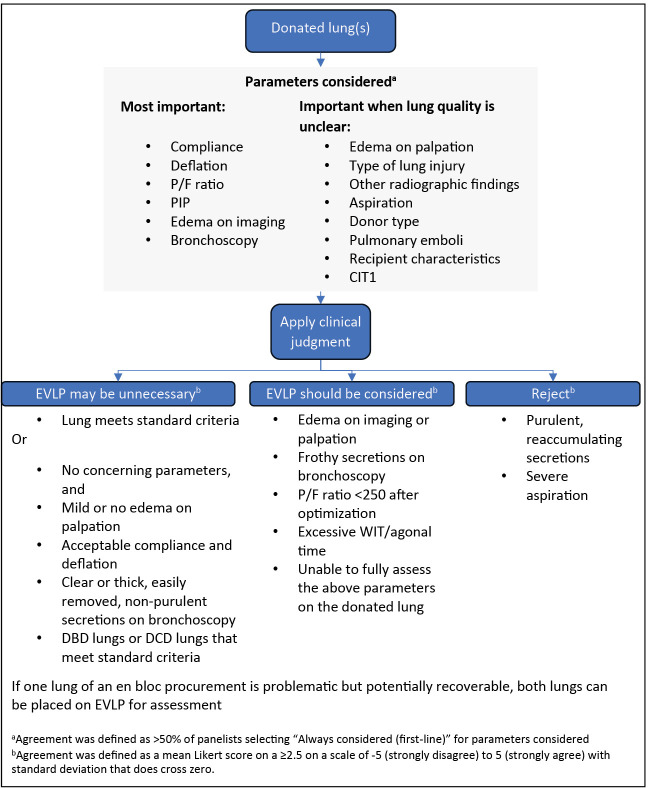
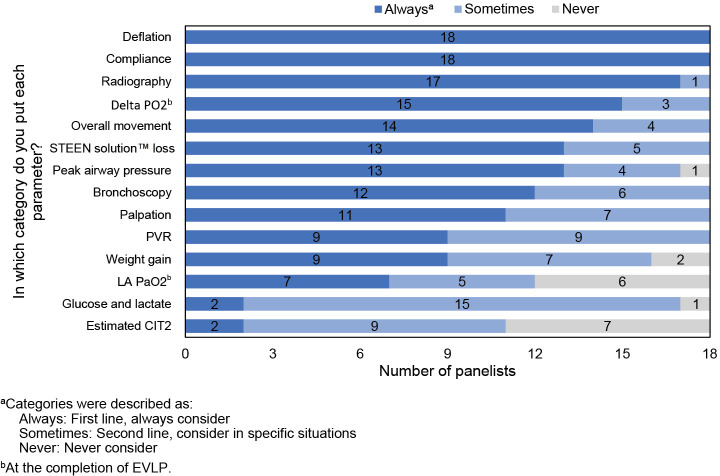
The primary goal for EVLP is expanding the number of donor lungs available for transplant. Lungs that are acceptable after EVLP are equivalent to lungs that met standard criteria initially. Lungs with unclear or marginal quality should be placed on EVLP for evaluation, including lungs received from third party organizations with incomplete or concerning information. Decisions on whether to put lungs on EVLP require nuanced clinical judgement and should consider compliance and deflation, the ratio of PaO2 to fraction of inspired oxygen (P/F ratio), peak inspiratory pressure (PIP), edema on imaging, and bronchoscopy, with additional parameters considered as appropriate if lung quality is unclear. EVLP lungs are appropriate for transplant if all relevant parameters are acceptable and may be appropriate if some parameters are borderline depending on clinical judgment. Decisions about transplanting EVLP lungs should consider radiography, delta PO2, overall movement, STEEN Solution™ loss, bronchoscopy, peak airway pressure, and palpation, along with other parameters as appropriate. Key open areas for research include evidence-based criteria for lung selection and assessment, the role of biomarkers, and enhanced techniques and perfusion solutions. In addition, the role of EVLP is unclear in lungs with pulmonary emboli and lungs procured with normothermic regional perfusion (NRP), as is the maximal duration of cold ischemia time (CIT).
Decisions about EVLP require nuanced consideration of numerous parameters. Expert opinion from this study may help optimize use of EVLP.
对原本不适合移植的供肺进行体外肺灌注(EVLP)可提供与标准标准肺移植相似的结果,并且据报道在一些移植中心可使移植量增加约20%。支持关于使用EVLP决策的证据有限,因此专家意见可能是一种有用的决策辅助工具。本研究使用改良的德尔菲法制定了关于使用无细胞灌注液进行EVLP的专家共识建议。
由18名在北美从事肺移植和EVLP的医生组成的小组完成了三项关于EVLP的调查:调查1使用开放式问题;调查2主要使用李克特量表问题;调查3重复调查2,同时向小组成员提供调查2的结果。调查3后的一次后续会议探讨了开放性问题。
EVLP的主要目标是增加可用于移植的供肺数量。经EVLP后可接受的肺等同于最初符合标准标准的肺。质量不明确或边缘的肺应进行EVLP评估,包括从第三方组织接收的信息不完整或令人担忧的肺。关于是否将肺置于EVLP上的决策需要细致入微的临床判断,应考虑顺应性和放气、动脉血氧分压与吸入氧分数之比(P/F比)、吸气峰压(PIP)、影像学上的水肿和支气管镜检查,如果肺质量不明确,则酌情考虑其他参数。如果所有相关参数均可接受,EVLP肺适合移植,如果某些参数处于临界值,根据临床判断也可能适合。关于移植EVLP肺的决策应考虑放射学、氧分压差值、整体运动、STEEN Solution™损失、支气管镜检查、气道峰压和触诊,以及酌情考虑的其他参数。关键的开放研究领域包括基于证据的肺选择和评估标准、生物标志物的作用以及改进的技术和灌注液。此外,EVLP在伴有肺栓塞的肺和通过常温区域灌注(NRP)获取的肺中的作用尚不清楚,冷缺血时间(CIT)的最长持续时间也是如此。
关于EVLP的决策需要对众多参数进行细致入微的考虑。本研究的专家意见可能有助于优化EVLP的使用。